- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
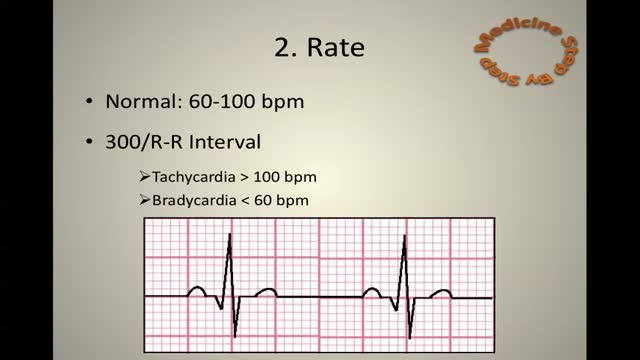
ECG Learn it

Watch that Full Human Dead Body Decomposing Video

Funny Video from hospital waiting room
Acute Myocardial Infarction - Heart Attack

Clinical Examination - Gait, Arms, Legs, Spine

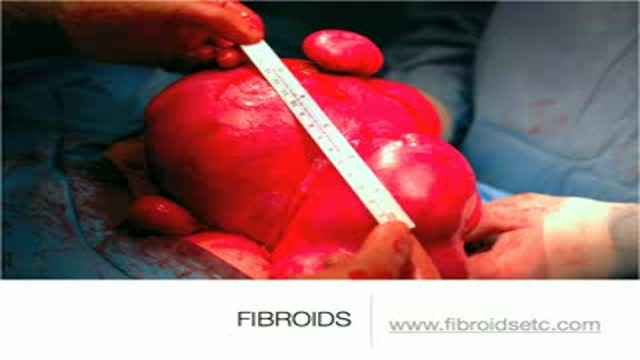
A uterine fibroid (also uterine leiomyoma, myoma, fibromyoma, leiofibromyoma, fibroleiomyoma, and fibroma) (plural of ... myoma is ...myomas or ...myomata) is a benign (non-cancerous) tumor that originates from the smooth muscle layer (myometrium) and the accompanying connective tissue of the uterus. Fibroids are the most common benign tumors in females and typically found during the middle and later reproductive years. While most fibroids are asymptomatic, they can grow and cause heavy and painful menstruation, painful sexual intercourse, and urinary frequency and urgency. Uterine fibroids is the major indication for hysterectomy in the US.[2] Fibroids are often multiple and if the uterus contains too many leiomyomatas to count, it is referred to as uterine leiomyomatosis. The malignant version of a fibroid is uncommon and termed a leiomyosarcoma.

Pulmonary edema is almost always treated in the emergency room or hospital. You may need to be in an intensive care unit (ICU). Oxygen is given through a face mask or tiny plastic tubes are placed in the nose. A breathing tube may be placed into the windpipe (trachea) so you can be connected to a breathing machine (ventilator) if you cannot breathe well on your own. The cause of edema should be identified and treated quickly. For example, if a heart attack has caused the condition, it must be treated right away. Medicines that may be used include: Diuretics that remove excess fluid from the body Medicines that strengthen the heart muscle, control the heartbeat, or relieve pressure on the heart
Lichen sclerosus is a skin condition that mainly affects the genital skin (vulva) in women and the penis in men. It most commonly occurs in middle-aged women. Symptoms may include itch, soreness, and changes in the appearance of affected skin.
Embolization is a medical advance that shrinks uterine fibroids. One tiny incision allows us to solve the problem quickly, safely and without surgery

Epilepsy surgery is reserved for people whose seizures are not well controlled by seizure medicines. This situation is sometimes called being "medically refractory" or "drug resistant." In children, the definition of medically refractory is even more individualized to the specific child's situation. Surgery may be considered for some children after weeks to months of treatment with seizure medicines.

Dr. Linder is removing a patients breast implants after having five breast augmentations from three previous surgeons. She has baker 4 capsular contracture and is look forward to having them removed. The most common reasons for removing a breast implant include; heath reasons such as back pain, reoccurring complications and the desire for a different shape or size. For implant removal surgery, Dr. Linder makes an inframammary incision (along the breast crease). The implant can be removed intact, or it may need to be punctured before removal. An antibiotic solution is used to irrigate the breast pocket after implant removal. For more information about breast implant removal go to www.implantremoval.net or call Dr. Linder's office at 310-275-4513

Penile Injection Therapy

Ingrown Hair Removal Video

This animated video will run you through the process of nuclear stress test.
Arterial Blood Gas Sampling

his patient had spilled boiling water on his lower leg a couple days before. This isn't complicated but the teaching points should focus on draining the large blistered areas and attempting to maintain moisture as long as we can so the skin doesn't contract down on itself.

Detailed examination of the joints is usually not included in the routine medical examination. However, joint related complaints are rather common, and understanding anatomy and physiology of both normal function and pathologic conditions is critically important when evaluating the symptomatic patient. By gaining an appreciation for the basic structures and functioning of the joint, you'll be able to "logic" your way thru the exam, even if you can't remember the eponym attached to each specific test!
A herniated disk refers to a problem with one of the rubbery cushions (disks) between the individual bones (vertebrae) that stack up to make your spine. A spinal disk is a little like a jelly donut, with a softer center encased within a tougher exterior. Sometimes called a slipped disk or a ruptured disk, a herniated disk occurs when some of the softer "jelly" pushes out through a crack in the tougher exterior. A herniated disk can irritate nearby nerves and result in pain, numbness or weakness in an arm or leg. On the other hand, many people experience no symptoms from a herniated disk. Most people who have a herniated disk don't need surgery to correct the problem.

Microsurgical bipolar cautery tonsillectomy compares favorably with traditional techniques in terms of intraoperative bleeding, postoperative pain, otalgia, and hemorrhage. This technique combines the hemostatic advantage of cautery dissection, the excellent visualization achieved by a microscope, and, with the use of a video, greatly improves the physician's ability to teach how to perform a tonsillectomy.
