- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
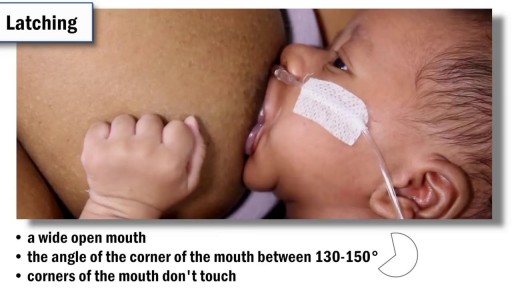
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
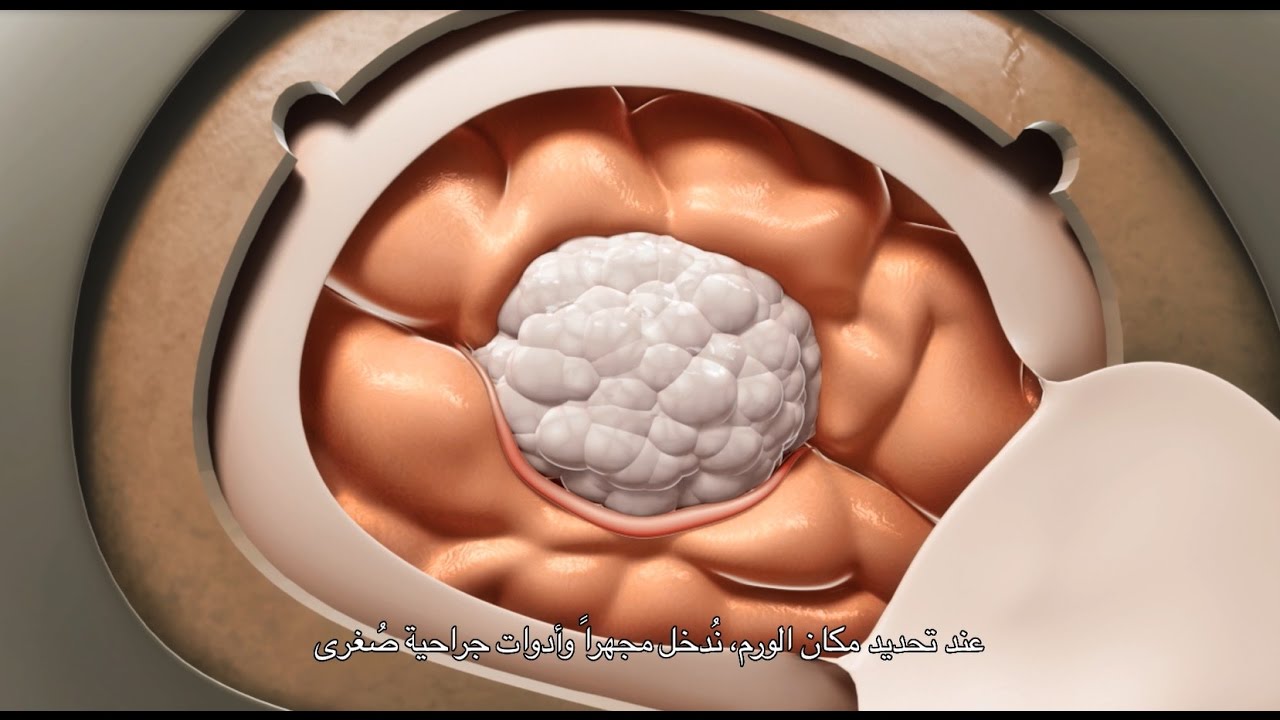
A craniotomy may be performed to treat brain tumors, blood clots, aneurysms, skull fractures, foreign objects, swelling of the brain, stroke or infection.


Brain port surgery is a minimally invasive surgical technique performed through a specially designed tube about the size of a dime. Using neuronavigation GPS-like guidance, the brain port is inserted into the brain with millimeter accuracy and is used as a channel to guide the surgeon and his/her instruments to various regions of the brain. Colloid cysts, metastatic tumors, and a variety of tumors within the ventricles are often candidates for this approach.

Pinch air out of the tip of the condom. Unroll condom all the way down the penis. After sex but before pulling out, hold the condom at the base. Then pull out, while holding the condom in place. Carefully remove the condom and throw it in the trash.
Watch that Female Foley Catheter Insertion Procedure
Peripheral Vascular Examination OSCE - Clinical Skills - Dr Gill
In the cardiovascular examination, particularly in the case of an OSCE station, we conclude the examination often by stating that the examiner would want to perform:
- An ECG
- Check full blood count
- and "do a peripheral vascular examination
In this video, we demonstrate that oft-talked about, but comparatively less common examination.
Starting off, with the examination of the hands, the radial, brachial and carotid pulses. before moving down to assess for a AAA, checking the femoral and popliteal pulses, before wrapping up around the ankle with the posterior tibial and dorsalis pedis pulses
For completeness, the cardiovascular examination is demonstrated here
https://www.youtube.com/watch?v=ECs9O5zl6XQ&t=2s
#PeripheralVascular #ClinicalSkills #DrGill

UPDATE 2/6/15: A new version of this animation is now available! https://www.youtube.com/watch?v=E1ljClS0DhM
This 3D medical animation depicts the surgical removal of the appendix (appendectomy) using laparoscopic instruments. The surgery animation begins by showing an inflamed appendix (appendicitis), followed by the placement of the laparoscope. Afterward, one can see the surgical device staple, cut and remove the inflamed appendix. Following the removal of the appendix the abdomen is flushed with a sterile saline solution to ensure all traces of infection have been removed.
ANCE00183

As a pediatric surgeon at NewYork-Presbyterian/Weill Cornell Medical Center, Dr. Nitsana Spigland treats newborns, children, teens, and young adults requiring surgical interventions. She specializes in antenatal counseling and newborn congenital malformations.
Learn more about Dr. Spigland at: https://www.nyp.org/physician/nspigland.
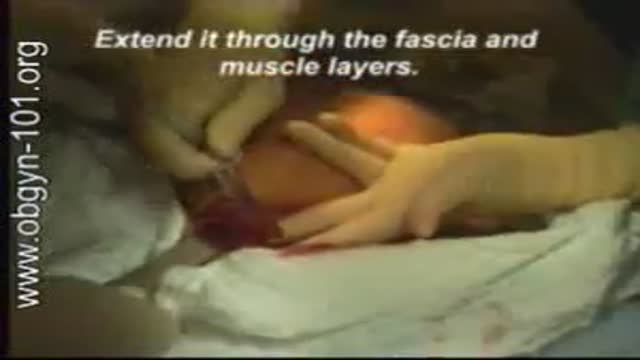
At one time, women who had delivered by cesarean section in the past would usually have another cesarean section for any future pregnancies. The rationale was that if allowed to labor, many of these women with a scar in their uterus would rupture the uterus along the weakness of the old scar. Over time, a number of observations have become apparent: Most women with a previous cesarean section can labor and deliver vaginally without rupturing their uterus. Some women who try this will, in fact, rupture their uterus. When the uterus ruptures, the rupture may have consequences ranging from near trivial to disastrous. It can be very difficult to diagnose a uterine rupture prior to observing fetal effects (eg, bradycardia). Once fetal effects are demonstrated, even a very fast reaction and nearly immediate delivery may not lead to a good outcome. The more cesarean sections the patient has, the greater the risk of subsequent rupture during labor. The greatest risk occurs following a “classical” cesarean section (in which the uterine incision extends up into the fundus.) The least risk of rupture is among women who had a low cervical transverse incision. Low vertical incisions probably increase the risk of rupture some, but usually not as much as a classical incision. Many studies have found the use of oxytocin to be associated with an increased risk of rupture, either because of the oxytocin itself, or perhaps because of the clinical circumstances under which it would be contemplated. Pain medication, including epidural anesthetic, has not resulted greater adverse outcome because of the theoretical risk of decreasing the attendant’s ability to detect rupture early. The greatest risk of rupture occurs during labor, but some of the ruptures occur prior to the onset of labor. This is particularly true of the classical incisions. Overall successful vaginal delivery rates following previous cesarean section are in the neighborhood of 70 This means that about 30of women undergoing a vaginal trial of labor will end up requiring a cesarean section. Those who undergo cesarean section (failed VBAC) after a lengthy labor will frequently have a longer recovery and greater risk of infection than had they undergone a scheduled cesarean section without labor. Women whose first cesarean was for failure to progress in labor are only somewhat less likely to be succesful in their quest for a VBAC than those with presumably non-recurring reasons for cesarean section. For these reasons, women with a prior cesarean section are counseled about their options for delivery with a subsequent pregnancy: Repeat Cesarean Section, or Vaginal Trial of Labor. They are usually advised of the approximate 70successful VBAC rate (modified for individual risk factors). They are counseled about the risk of uterine rupture (approximately 1in most series), and that while the majority of those ruptures do not lead to bad outcome, some of them do, including fetal brain damage and death, and maternal loss of future childbearing. They are advised of the usual surgical risks of infection, bleeding, anesthesia complications and surgical injury to adjacent structures. After counseling, many obstetricians leave the decision for a repeat cesarean or VBAC to the patient. Both approaches have risks and benefits, but they are different risks and different benefits. Fortunately, most repeat cesarean sections and most vaginal trials of labor go well, without any serious complications. For those choosing a trial of labor, close monitoring of mother and baby, with early detection of labor abnormalities and preparation for

Traditional Liposuction VS Vaser Liposuction
A side-by-side comparison of traditional liposuction and a #Vaser liposuction. Both of these were performed by our skilled surgeons at Divine Cosmetic Surgery.
#vaserliposuction #liposuction #liposuctionDelhi #liposuctionresults #shorts #vaserliposuctionDelhi
Know more about liposuction
https://www.divinecosmeticsurg....ery.com/liposuction-
Traditional Liposuction vs 360 High Def Vaser Liposuction - https://www.youtube.com/watch?v=r_bBI2p9fVI&t=14s
-------------------------------------------------------------------------------
Why Vaser Is Best For Thigh Liposuction - https://youtu.be/dlzpdDEZcS4
-------------------------------------------------------------------------------
Abdomen Vaser Liposuction - Live - https://www.youtube.com/watch?v=_Cvl2Txn8LQ
-------------------------------------------------------------------------------
Back Vaser Liposuction In Female - https://youtu.be/OC60UdgtIWU
-------------------------------------------------------------------------------
For more details about Liposuction Visit - https://www.divinecosmeticsurgery.com/
-------------------------------------------------------------------------------
Dr. Amit Gupta
MBBS, M.S., DNB (Plastic & Cosmetic Surgery)
Divine Cosmetic Surgery | +91 9811994417
info@divinecosmeticsurgery.com | 01141828787
Delhi | Mumbai | Gurgaon
𝗦𝗼𝗰𝗶𝗮𝗹 𝗠𝗲𝗱𝗶𝗮 𝗮𝗻𝗱 𝗬𝗼𝘂𝘁𝘂𝗯𝗲 𝘃𝗶𝗱𝗲𝗼 𝗰𝗵𝗮𝗻𝗻𝗲𝗹 : -
🎦 https://www.youtube.com/c/DrAm....itGuptaBestPlasticCo
👍🏻 https://www.facebook.com/dramitguptaplasticsurgeon
📷 https://www.instagram.com/divineaesthetics_delhi/
🐥 https://twitter.com/dramitguptajee
🖇️ https://www.linkedin.com/compa....ny/divinecosmeticsur
📌 https://pinterest.com/divinesurgery
#Liposuction #vaserliposuction #liposuctioncostinindia #liposuctiondelhi #liposuction #liposuctioncost #liposuctioncostfactors #liposuctioncostindelhi #DrAmitGuptaPlasticSurgeon #DivineCosmeticSurgery #dramitgupta
Disclaimer: The information on our videos & social media is provided for informational purposes only and is not meant for the advice provided by your surgeon.
We are not responsible for any harm if anyone misguides you from our name. Our all-social media official handles are linked up on our website. All images & content used on our videos & social media are for illustrative concerns only, original results and processes may vary.

Our General Surgery team treats hernia patients on a daily basis. In fact, you could consider them to be hernia experts. We sat down with one of those experts, Dr. Heater Dunlap, to talk about the common signs and symptoms of hernias and to answer the question of when to see a doctor.


Site enhancement oil, often called "santol" or "synthol" (no relation to the Synthol mouthwash brand), refers to oils injected into muscles to increase the size or change the shape. Some bodybuilders, particularly at the professional level, inject their muscles with such mixtures to mimic the appearance of developed muscle where it may otherwise be disproportionate or lagging. This is known as "fluffing".Synthol is 85% oil, 7.5% lidocaine, and 7.5% alcohol. It is not restricted, and many brands are available on the Internet. The use of injected oil to enhance muscle appearance is common among bodybuilders, despite the fact that synthol can cause pulmonary embolisms, nerve damage, infections, sclerosing lipogranuloma,[60] stroke,[55] and the formation of oil-filled granulomas, cysts or ulcers in the muscle. Rare cases might require surgical intervention to avoid further damage to the muscle and/or to prevent loss of life. Sesame oil is often used in such mixtures, which can cause allergic reactions such as vasculitis.
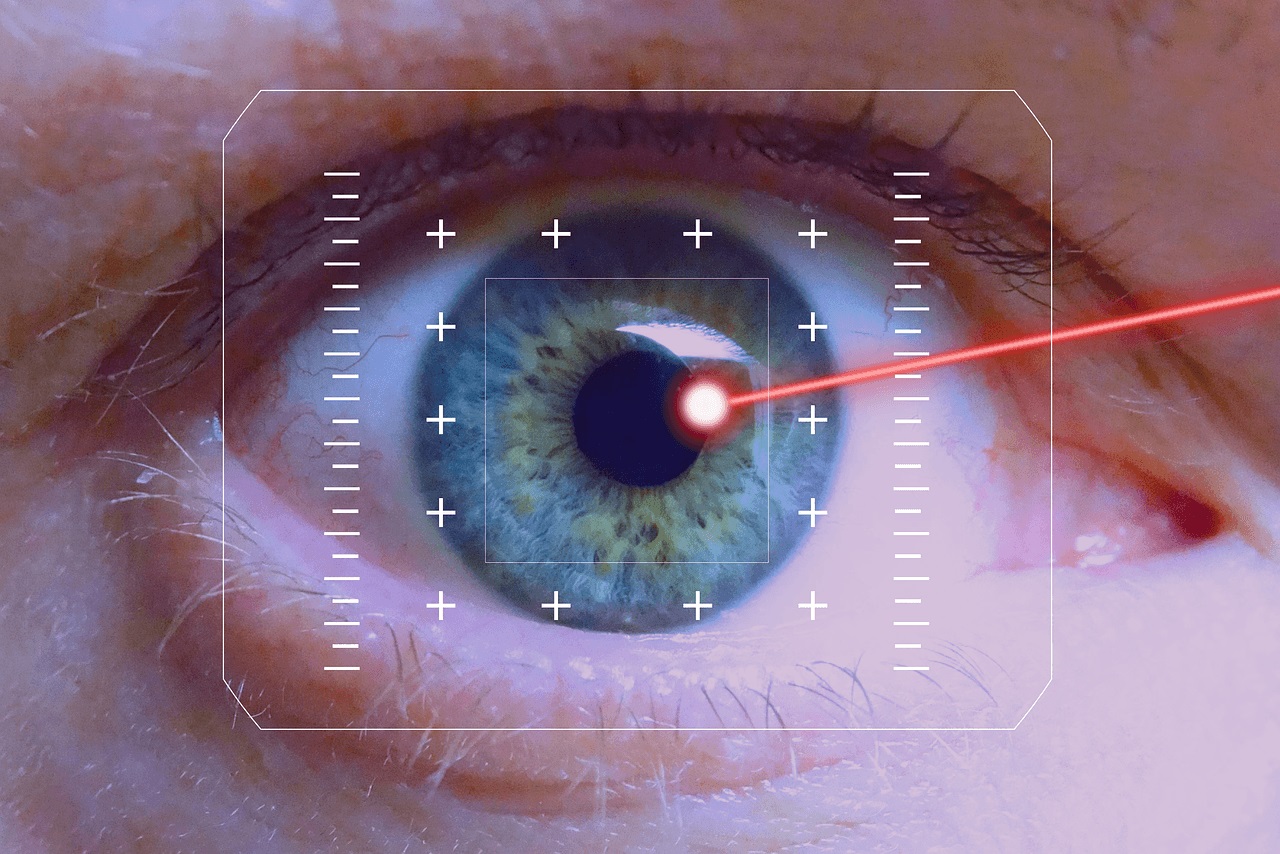
LASIK eye procedure for correcting vision

This is an educational medical video for Medical Students showing how to examine a hernia swelling

28 years old gentleman presented with huge liver abscess in the right lobe, with repeated attempts of percutaneous aspirations in the past. He was evaluated and subjected to Laparoscopic drainage. This video depicts feasibility of laparoscopy in deep seated liver abscesses. Video created by: Dr. Juneed M. Lanker Fellow Minimal Access Surgery Apollo Hospitals Chennai.

Watch that Skin Jiggers Removal Procedure
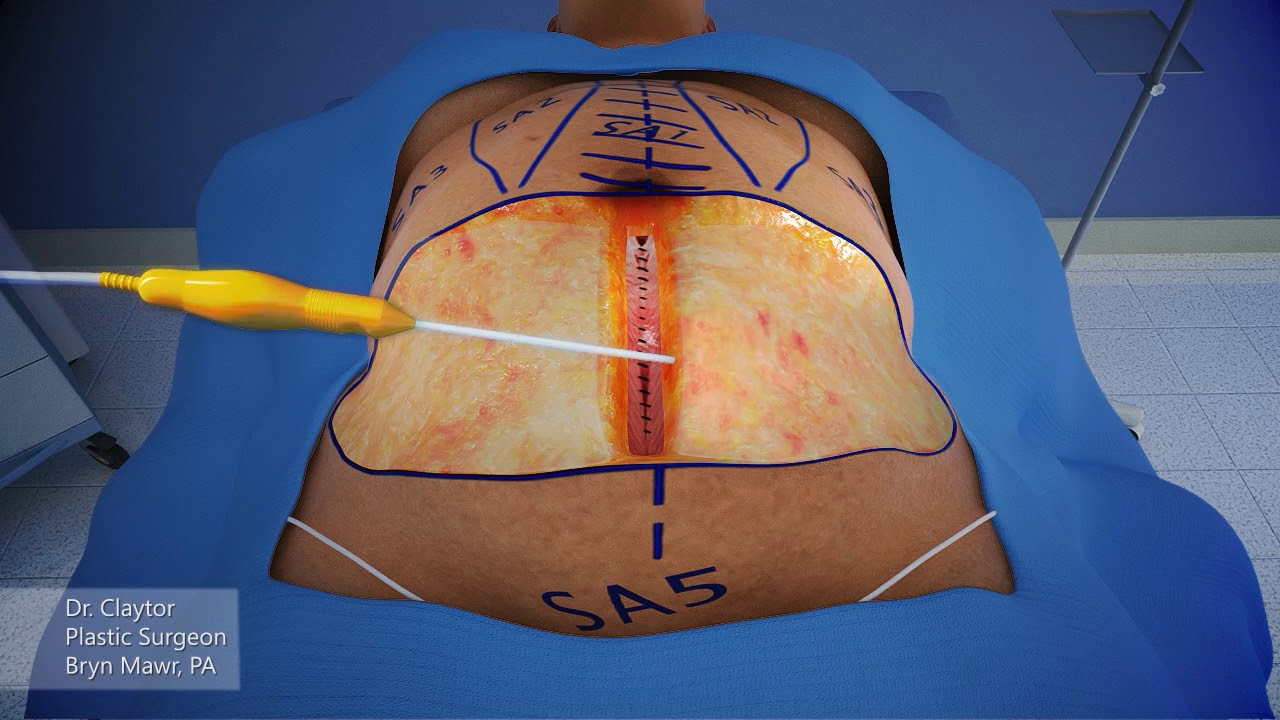
Dr. Claytor uses a 3-D animation to demonstrate how a drainless tummy tuck combined with liposuction can effectively reduce excess skin and fat on the abdomen WITHOUT the need for drains during post-op recovery!
Learn more about Dr. Claytor’s drainless tummy tucks here: https://www.cnplasticsurgery.c....om/procedures/body/t
R. Brannon Claytor, MD, FACS is a renowned double board-certified plastic surgeon and director of Claytor Noone Plastic Surgery, a premium plastic surgery practice in Bryn Mawr, PA that proudly serves the Philadelphia, Main Line, and surrounding areas. Dr. Claytor’s superb skill and results have been recognized for over a decade, earning him numerous awards in both local and national publications, including Philadelphia Magazine, Main Line Today, and Newsweek.
Together, Dr. Claytor and his experienced aesthetics team provide a variety of surgical and non-surgical procedures for the face, breasts, and body to help you look and feel your best. To learn more about how Dr. Claytor and our entire staff can help you reach your goals, please visit our website or give us a call at 610-527-4833.
About Dr. Claytor: https://www.cnplasticsurgery.c....om/our-practice/dr-r
Claytor Noone Plastic Surgery: https://www.cnplasticsurgery.com/
Essential guide to plastic surgery (procedures, costs, planning and more): https://www.cnplasticsurgery.c....om/our-practice/esse
Questions? Contact us online: https://www.cnplasticsurgery.com/contact-us/

A patient at a British hospital played Mahler and Gershwin on the violin while surgeons removed a tumor from her brain, so doctors could preserve her ability to play music.
She left the hospital 3 days later and hopes to return to the symphony soon. https://abcn.ws/2SGY9mp
SUBSCRIBE to ABC NEWS: https://www.youtube.com/ABCNews/
Watch More on http://abcnews.go.com/
LIKE ABC News on FACEBOOK
https://www.facebook.com/abcnews
FOLLOW ABC News on TWITTER:
https://twitter.com/abc
GOOD MORNING AMERICA'S HOMEPAGE:
https://www.goodmorningamerica.com/
