- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Permanent pacemaker insertion is considered a minimally invasive procedure. Transvenous access to the heart chambers under local anesthesia is the favored technique, most commonly via the subclavian vein, the cephalic vein, or (rarely) the internal jugular vein or the femoral vein.
The bladder is a hollow organ in the lower abdomen (pelvis). It collects and stores urine produced by the kidneys. The bladder is connected to the kidneys by a tube from each kidney called a ureter. When the bladder reaches its capacity of urine, the bladder wall contracts, although adults have voluntary control over the timing of this contraction. At the same time, a urinary control muscle (sphincter) in the urethra relaxes. The urine is then expelled from the bladder. The urine flows through a narrow tube called the urethra and leaves the body. This process is called urination, or micturition.
This animation describes the goals of inflammatory bowel disease (IBD) management and how patients can take an active role in managing their disease.

Take your left leg and place your ankle against the knee. Hold the position for a moment before changing legs. This helps stretch the tiny piriformis muscle, which sometimes becomes inflamed and presses against the sciatic nerve causing pain. Repeat by switching sides and doing the same exercise with the other leg.
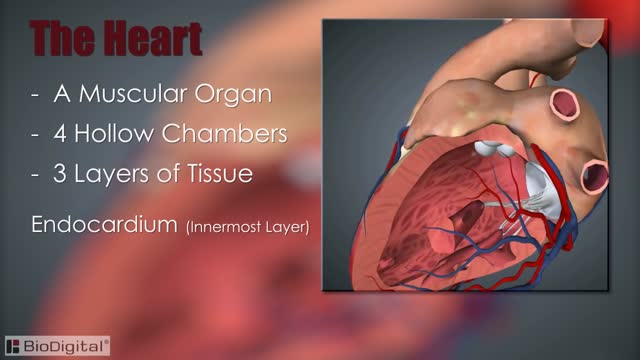
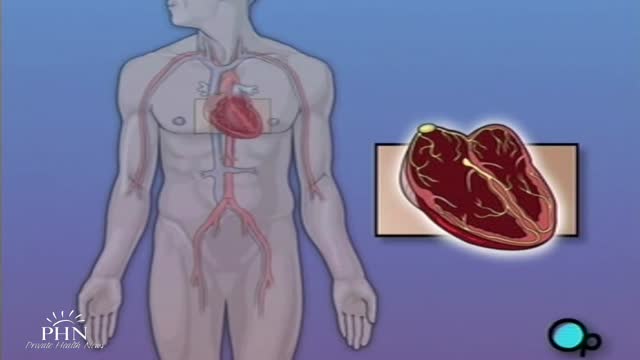
The heart, blood vessels, and blood are the parts that make up the circulatory system, which is defined as a closed system of blood vessels for the transport of gasses and nutrients. The heart is the key organ in the circulatory system. As a hollow, muscular pump, its main function is to propel blood throughout the body.
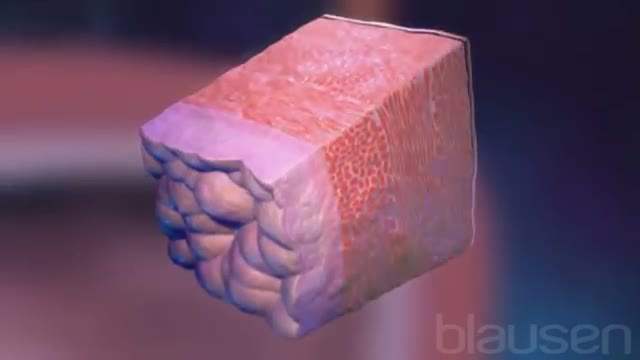
These air sacs make up most of the lung tissue. Lung diseases affecting the alveoli include: Pneumonia: An infection of the alveoli, usually by bacteria. Tuberculosis: A slowly progressive pneumonia caused by the bacteria Mycobacterium tuberculosis. Chronic respiratory diseases are chronic diseases of the airways and other structures of the lung. Some of the most common are: asthma, chronic obstructive pulmonary disease, occupational lung diseases and pulmonary hypertension.

Electrical Cardioversion
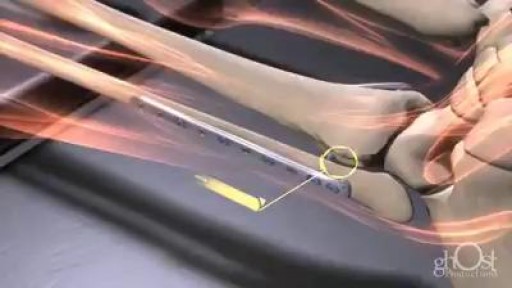
How Bone Fractures Are Repaired

Stephen has got the medical treatment at Asian Hip Resurfacing Surgical Center in india.
Dr.Vijay Bose (Orthopedic Consultant),
Asian Hip Resurfacing Surgical Center.
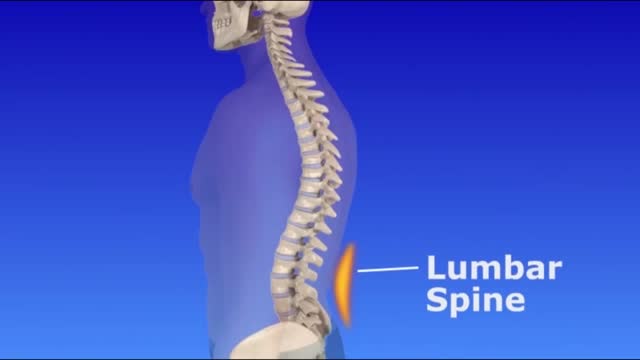
If you look at someone’s back, you’ll see that the spine runs straight down the middle. When a person has scoliosis, their backbone curves to the side. The angle of the curve may be small, large or somewhere in between. But anything that measures more than 10 degrees is considered scoliosis. Doctors may use the letters “C” and “S” to describe the curve of the backbone. You probably don’t look directly at too many spines, but what you might notice about someone with scoliosis is the way they stand. They may lean a little or have shoulders or hips that look uneven. What Causes Scoliosis? In as many as 80% of cases, doctors don’t find the exact reason for a curved spine. Scoliosis without a known cause is what doctors call “idiopathic.” Some kinds of scoliosis do have clear causes. Doctors divide those curves into two types -- structural and nonstructural. In nonstructural scoliosis, the spine works normally, but looks curved. Why does this happen? There are a number of reasons, such as one leg’s being longer than the other, muscle spasms, and inflammations like appendicitis. When these problems are treated, this type of scoliosis often goes away.

TUMMY TUCK 🤩 Immediate OR Results
This patient wanted to get her abs back, but unfortunately NO diet or workout can tighten muscles that have been stretched apart from carrying a baby 👀 But we can fix that at Lemmon Avenue Plastic Surgery & Laser Center!
To learn more about the #tummytuck click here: https://drdeuber.com/procedures/tummy-tuck/
For #mommymakeover, click here: https://drdeuber.com/procedures/mommy-makeover/
👙
#MarkDeuberMD

Angioplasty Procedure Animation

Video shows a Hip resurfacing operation done using the Durom hip from Zimmer.
The patient is a young active male. Hip resurfacing is emerging as the surgical procedure of choice in young and active patients for pain relief from Hip arthritis.
Blind loop syndrome (BLS), commonly referred to in the literature as small intestinal bacterial overgrowth (SIBO) or bacterial overgrowth syndrome (BOS), is a state that occurs when the normal bacterial flora of the small intestine proliferates to numbers that cause significant derangement to the normal physiological ...

A high definition medical video showing the Laparoscopic inguinal hernia repair

When it comes to our health men over the age of 45 are in need of regular doctor visits and testing, as a large percentage of medical decisions are based on the lab test results.

- elbow dislocations in children are a relatively uncommon; - peak incidence occurs in adolescence between 11-15 years. - posterior dislocations are most common type; - posterior dislocation usually results from fall on outstretched hand w/ forarm supinated & elbow extended or partially flexed; - coronoid process, which nl resists posterior displacement of ulna, is relatively small in children; - anterior capsule of elbow joint is torn by force of the impact transmitted upward thru the ulna and radius
Acute kidney failure — also called acute renal failure or acute kidney injury — develops rapidly over a few hours or a few days. Acute kidney failure is most common in people who are already hospitalized, particularly in critically ill people who need intensive care. Acute kidney failure can be fatal and requires intensive treatment. However, acute kidney failure may be reversible. If you're otherwise in good health, you may recover normal or nearly normal kidney function

Anatomy of The Ear

Anatomy of Anterior Abdominal Wall
