- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Keratoderma Blennorrhagicum is a manifestation on the skin that appears in patients diagnosed with reactive arthritis (this condition was previously known as Reiter syndrome). The condition manifests itself by lesions that appear on the skin, initially on the palm of the hands and soles of the feet. The lesions have the tendency to spread, affecting other parts of the body, such as the scrotum, scalp or trunk. Because of their appearance, the lesions might be easily confused with the ones from psoriasis. Keratoderma blennorrhagicum is one of the symptoms that can be used for the clinical diagnosis of reactive arthritis.
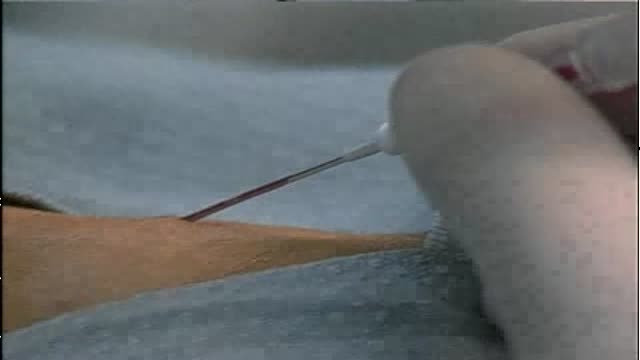
In human anatomy, the radial artery is the main blood vessel, with oxygenated blood, of the lateral aspect of the forearm.
NTIS refers to a syndrome found in seriously ill or starving patients with low fT3, usually elevated RT3, normal or low TSH, and if prolonged, low fT4. It is found in a high proportion of patients in the ICU setting, and correlates with a poor prognosis if TT4 is <4ug/dl. The patho-physiology includes suppression of TRH release, reducedT3 and T4 turnover, reduction in liver generation of T3, increased formation of RT3, and tissue specific down-regulation of deiodinases, transporters, and TH receptors. Although long debated, tissue TH levels are definitely reduced, and tissue hypothyroidism is presumably present. This is often not clinically evident because of the brief duration, and reduced but not absent tissue levels of TH. Although recognized for nearly 4 decades, interpretation of the syndrome is contested, because of lack of data. Some observes, totally without data, argue that it is a protective response and should not be treated. Other observers (as in this review) present available data suggesting, but not proving, that thyroid hormone replacement is appropriate, not harmful, and may be beneficial. The best form of treatment (TRH,TSH,or T3+T4) and possible accompanying treatments (GHRH, Cortisol, nutrition, insulin) lack consensus. In this review current data are laid out for reader’s review and judgment.

Wound-closure technologies are becoming less painful and more efficient at closing wounds

Most retinal tears need to be treated by sealing the retina to the back wall of the eye with laser surgery or cryotherapy (a freezing treatment). Both of these procedures create a scar that helps seal the retina to the back of the eye. This prevents fluid from traveling through the tear and under the retina, which usually prevents the retina from detaching. These treatments cause little or no discomfort and may be performed in your ophthalmologist’s office. With laser surgery, your ophthalmologist uses a laser to make small burns around the retinal tear. The scarring that results seals the retina to the underlying tissue, helping to prevent a retinal detachment.

Aspirin, or acetylsalicylic acid (ASA) is a salicylate drug, and is generally used as an analgesic (something that relieves pain without producing anesthesia or loss of consciousness) for minor aches and pains, to reduce fever (an antipyretic), and also as an anti-inflammatory drug.
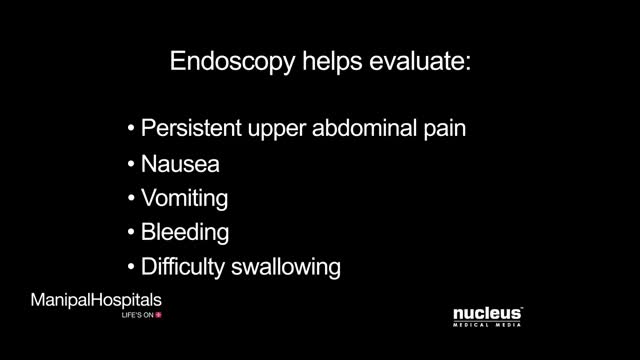
This animated video is an informative video that provides information regarding Upper Gastro-intestinal Endoscopy. An upper GI endoscopy procedure allows your doctor to view the mucus lining of the upper portion of your gastro-intestinal tract. This includes your oesophagus, stomach and duodenum. Upper endoscopy is used to evaluate symptoms of persistent upper abdominal pain, nausea, vomiting, bleeding, or difficulty in swallowing. The procedure is performed using an endoscope which is a long thin flexible tube a light and a tiny video camera attached to the end. The camera transmits the image to a monitor. Uncomplicated upper endoscopy takes 10-20 minutes, your doctor will gently insert the endoscope through your mouth and then slowly and carefully move it down your oesophagus until it reaches your stomach. An endoscopy for stomach may also be necessary in some cases.
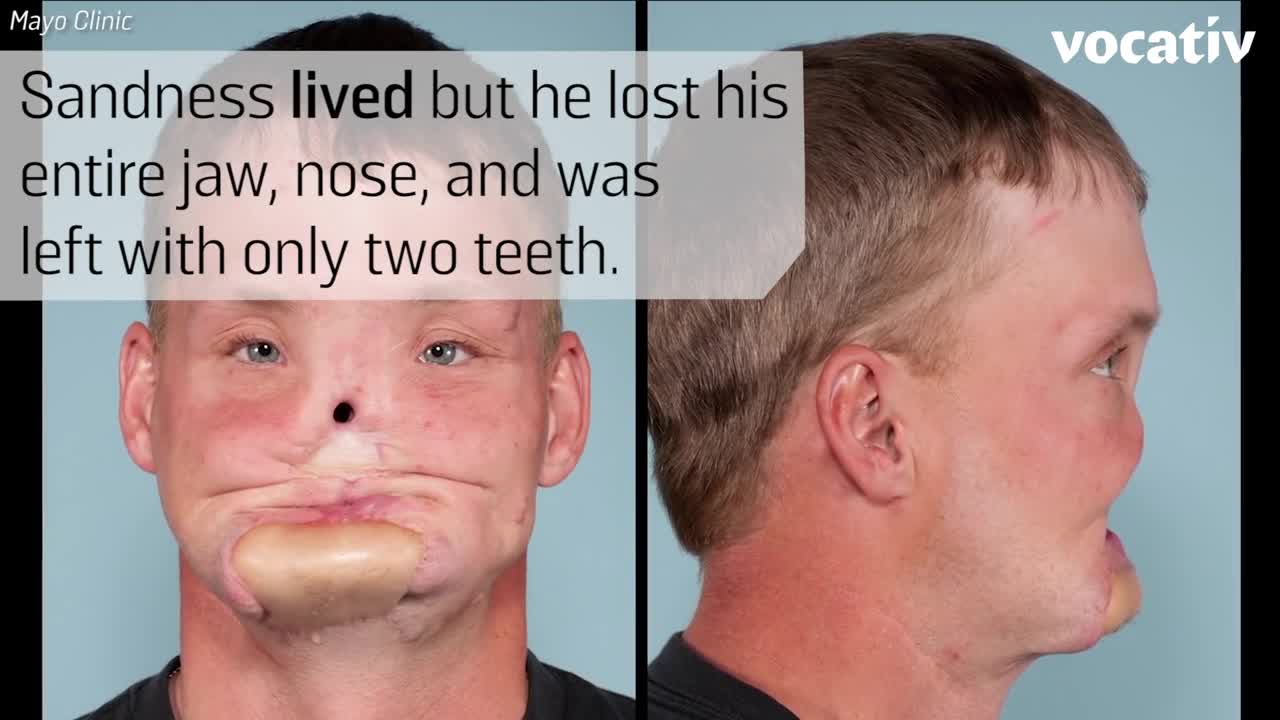
Doctors at the Mayo Clinic used 3D-printed models to prepare for their first-ever face transplant.
Lumbar Laminotomy and Microdiscectomy

Womb Fight amazing

Colon - Polypectomy, Saline lift, Adenomas
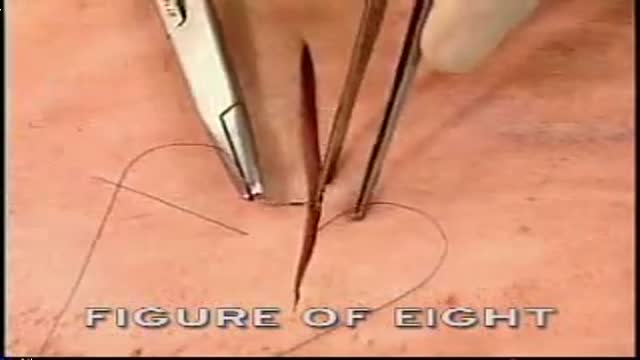
Figure of Eight 8 Suture

Hepatitis C is an infection caused by the hepatitis C virus (HCV) that attacks the liver and leads to inflammation. The World Health Organization (WHO) estimates that about 3% of the world’s population has been infected with HCV and that there are more than 170 million chronic carriers who are at risk of developing liver cirrhosis and/or liver cancer. The image below depicts the HCV genome.
In this video, Dr. Joe Bresee, with the CDC Influenza Division, describes swine flu - its signs and symptoms, how it's transmitted, medicines to treat it, steps people can take to protect themselves from it, and what people should do if they become ill.

Video giving an overview of histology, slide preparation, histological stains, and types of microscopy. This video is a part of our Histology Video Course (https://youtube.com/playlist?l....ist=PLnr1l7WuQdDynxT
Specific topics: what is histology, general composition of tissues, histotechnology: how histology slides are prepared, histology stains, immunohistochemistry, light microscopy vs electron microscopy, and pro tips for learning histology
Additional YouTube Content
Anatomy Videos: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDz2dK
Biochemistry videos: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDzCUC
DaVinci Cases Videos: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDyJUl
The DaVinci Hour Podcast: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDwSm9
DaVinci Academy Website: https://www.dviacademy.com/

The eyelid is injected with a local anesthetic, a clamp is put on the eyelid, then the eyelid is turned over, an incision is made on the inside of the eyelid, and the chalazion is drained and scraped out with a curette. A scar on the upper lid can cause discomfort as some patients feel the scar as they blink.

Watch that video to know How to Remove Teeth Plaque Naturally

Diverticula are small, bulging pouches that can form in the lining of your digestive system. They are found most often in the lower part of the large intestine (colon). Diverticula are common, especially after age 40, and seldom cause problems. Sometimes, however, one or more of the pouches become inflamed or infected. That condition is known as diverticulitis (die-vur-tik-yoo-LIE-tis). Diverticulitis can cause severe abdominal pain, fever, nausea and a marked change in your bowel habits. Mild diverticulitis can be treated with rest, changes in your diet and antibiotics. Severe or recurring diverticulitis may require surgery.

DMC Neurosurgeon Sandeep Mittal uses EEG and brain surgery to decode the secrets of adult epilepsy - Part I of a two-part series. ~ Detroit Medical Center

The journey of egg and sperm. There are a lot of casualties (deaths) among the sperm as they swim toward the egg. First, many get lost in the maze of a woman's uterus where they also have to contend with acidic vaginal secretions.
