- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
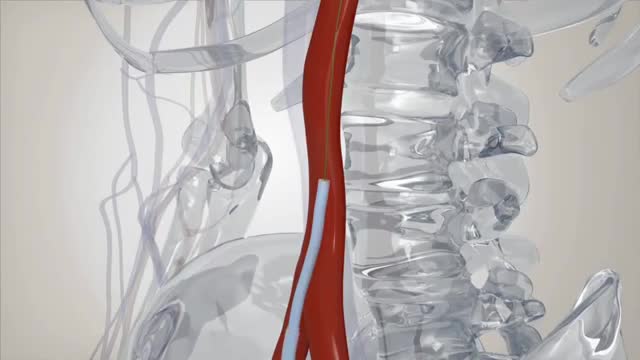
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A posterior Gastroenteral side to side anastomosis is presented. The procedure is made with circular stapler. After a good hemostasis of the suture has been obtained, the gastrotony is closed with linear stapler and running suture.

Total Hip Replacement Animation
Aortic valve replacement is a procedure in which a patient's failing aortic valve is replaced with an artificial heart valve. The aortic valve can be affected by a range of diseases; the valve can either become leaky (aortic insufficiency / regurgitation) or partially blocked (aortic stenosis).

No - Knife Endovenous Laser

For both DCIS and invasive cancer, radiation therapy to the remaining breast tissue is generally recommended after surgery. A lumpectomy may also be called breast-conserving surgery, a partial mastectomy, quadrantectomy, or a segmental mastectomy. A mastectomy is the surgical removal of the entire breast.
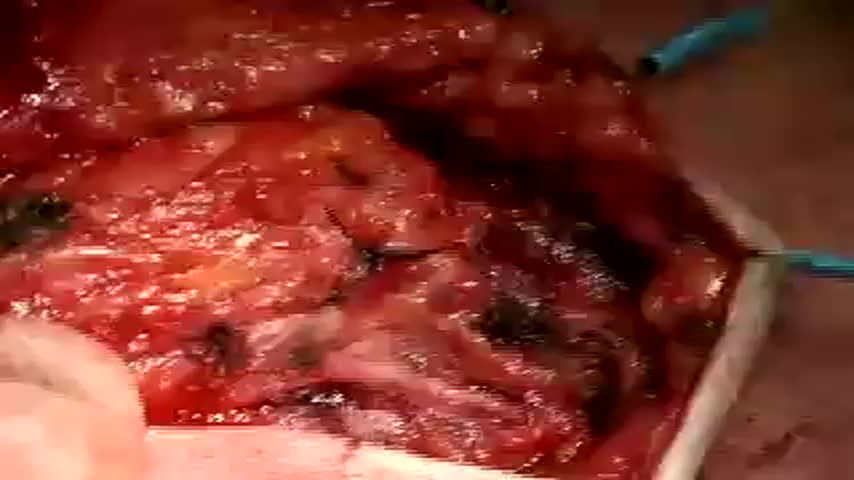
This video show the steps in a total parotidectomy with VII nerve preservation. The patient had a malignant parotid tumor without VII nerve compromise.

Diverticula are small, bulging pouches that can form in the lining of your digestive system. They are found most often in the lower part of the large intestine (colon). Diverticula are common, especially after age 40, and seldom cause problems. Sometimes, however, one or more of the pouches become inflamed or infected. That condition is known as diverticulitis (die-vur-tik-yoo-LIE-tis). Diverticulitis can cause severe abdominal pain, fever, nausea and a marked change in your bowel habits. Mild diverticulitis can be treated with rest, changes in your diet and antibiotics. Severe or recurring diverticulitis may require surgery.

Do I Need to See My Doctor for Menstrual Cramps? || Common gynaecological problems in women It's perfectly normal to experience mild cramps during your period, and the good news is that these cramps can usually be eased with simple therapies like a heating pad or an over-the-counter pain reliever. However, some women's menstrual cramps may not feel better with these basic remedies. If this is the case for you, making an appointment with your doctor is important. This way you not only get the pain relief you deserve but also ensure there is nothing else going on.
CDC's Dr. Joe Bresee describes how to prevent giving and getting novel H1N1 flu.

If you go to research LASIK eye surgery online, you may get conflicting messages. Some articles rave about it, but in some cases, others link it to severe pain or even suicide. 7 Action News' Carolyn Clifford sat down with one of the area's biggest providers of eye surgery to try and separate fact from fiction, so if you go under the laser, you know the risk.
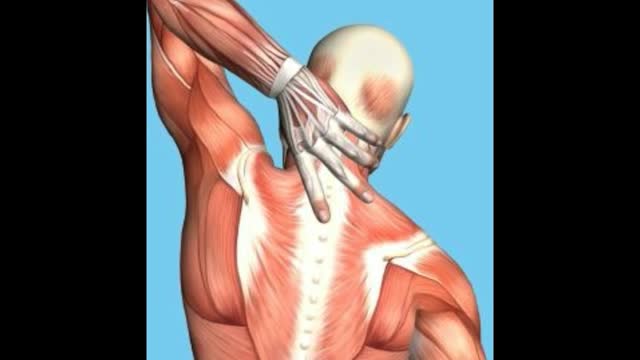
This video: Rhomboid muscle strain and spasm causes upper back pain between the shoulder blades. Some patients describe the muscle spasms and discomfort as knots in the back. Early treatment is important to speed healing and recovery. Ice therapy for the first few days followed by moist heat can help relieve symptoms.Oct 12, 2015
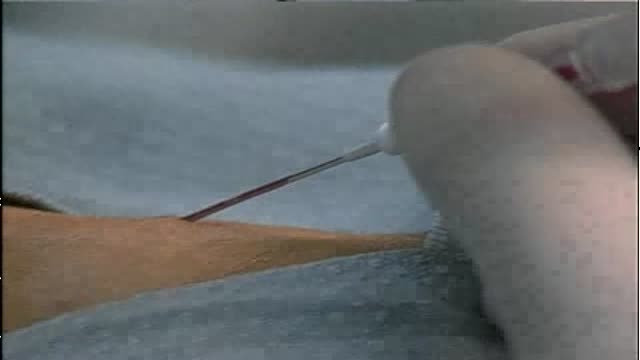
In human anatomy, the radial artery is the main blood vessel, with oxygenated blood, of the lateral aspect of the forearm.

arteriovenous hemodialysis access has been the "gold standard" for patients needing hemodialysis for the past 30 years. Despite the reported advantages of autologous access, the availability of prosthetic graft material, coupled with the challenging dialysis candidate, has led to a trend of primary prosthetic graft dialysis access in the 1980s and 1990s. In recognition of this unfortunate trend, the National Kidney Foundation Dialysis Outcomes Quality Initiative (DOQI) used evidence from published studies and summary articles to generate clinical practice guidelines, emphasizing a shift back to autologous arteriovenous fistula (AVF) as the key to long-term successful hemodialysis.[1,2] These initial guidelines proposed a goal of 50% autologous AVF as the initial access, with a 40% prevalence of autologous access for a given practice or unit.
Neuropathic pain: often difficult to treat. Palmitoylethanolamide (PEA) is a very special molecule, produced in our own body, against pain and chronic inflammation. PEA is available as supplement and as cream, and as dietfood for medical purposes in Italy and Spain. It has been explored since 1957 and has a clear analgesic and anti-inflammatory efficacy, and virtually no side effects. Meanwhile within the context of clinical trials 5000 patients have been using PEA, and its efficacy and safety has been documented in more than 400 scientific papers: http://palmitoylethanolamide4pain.com/about-2/ a website containing 400+ scientific articles on PEA in 6 different languages. The PEA datapool.

Knee replacement involves replacing a knee joint that has been damaged or worn away, usually by arthritis or injury. Find out more here: https://www.bupa.co.uk/health-....information/knee-cli
Medicine is advancing faster than ever and breakthroughs are happening right now at the Detroit Medical Center. ~ Detroit Medical Center

In a normal person, when a muscle tendon is tapped briskly, the muscle immediately contracts due to a two-neuron reflex arc involving the spinal or brainstem segment that innervates the muscle. The afferent neuron whose cell body lies in a dorsal root ganglion innervates the muscle or Golgi tendon organ associated with the muscles; the efferent neuron is an alpha motoneuron in the anterior horn of the cord. The cerebral cortex and a number of brainstem nuclei exert influence over the sensory input of the muscle spindles by means of the gamma motoneurons that are located in the anterior horn; these neurons supply a set of muscle fibers that control the length of the muscle spindle itself.

Originally broadcast November 21, 2014.
They advertise low, low prices. But does anyone actually pay that rate? Erica Johnson investigates.
More from CBC Marketplace, Canada's top consumer affairs show:
Watch episodes online at http://cbc.ca/marketplace
Like us on Facebook: http://facebook.com/cbcmarketplace
Talk to us on Twitter: http://twitter.com/cbcmarketplace
Follow our hosts @cbctom and @cbcerica

Detroit Medical Center commercial for Electronic Medical Record - DMC is the only healthcare system in Michigan with 100% medication scanning - a huge leap forward in patient safety. ~ Detroit Medical Center

Modified Milch method of relocating a dislocated shoulder
