- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

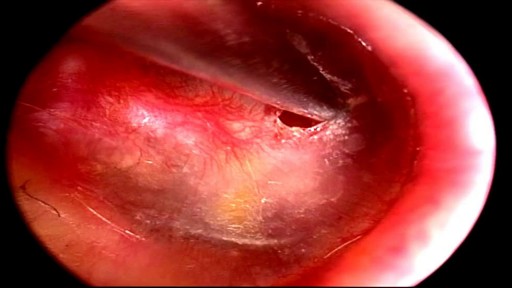
Central vestibular nystagmus results from stimulation, injury, disease of the central vestibular pathways of the brainstem or the cerebellum, or lesion of the vestibular nuclei. It is typically a jerk nystagmus, which can be purely horizontal, vertical or torsional.
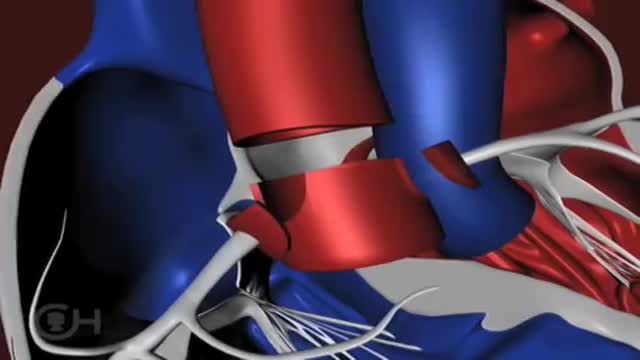
The "great arteries" in this anomaly refer to the aorta and the pulmonary artery, the two major arteries carrying blood away from the heart. In cases of transposition of the great arteries, these vessels arise from the wrong ventricle. They are "transposed" from their normal position so that the aorta arises from the right ventricle and the pulmonary artery from the left ventricle. Other heart defects may occur along with transposition of the great arteries. About 25 percent of children with transposition will also have a ventricular septal defect (VSD) . In nearly a third, the branching pattern of the coronary arteries as they leave the transposed aorta is unusual. Infants may also have narrowing below the pulmonary valve that blocks blood flow from the left ventricle to the lungs.

Splenectomy for massive splenomegaly (>1500 g) provides palliation but is associated with a high rate of perioperative complications in a population of patients with advanced hematological malignancies. Predictive factors for survival and whether the palliative goals are achieved in the long-term are not well defined.

DMC Specialists use minimally invasive surgery to remove an extremely large uterine fibroid from a patient. ~ Detroit Medical Center


The ABC's of Adult CPR
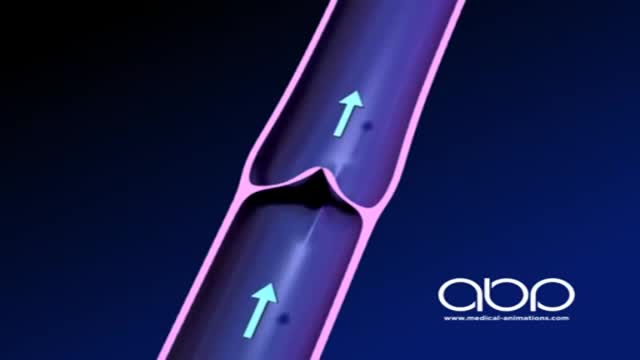
The deep veins play a significant role in propelling blood toward the heart. The one-way valves in deep veins prevent blood from flowing backward, and the muscles surrounding the deep veins compress them, helping force the blood toward the heart, just as squeezing a toothpaste tube ejects toothpaste.


Five percent of pregnant women have gestational diabetes, so if you're expecting, understanding the basics of this common condition is vital

Subtotal Thyroidectomy

Colonoscopy is a test that allows your doctor to look at the inner lining of your large intestine (rectum and colon). He or she uses a thin, flexible tube called a colonoscope to look at the colon. A colonoscopy helps find ulcers, colon polyps, tumors, and areas of inflammation or bleeding.
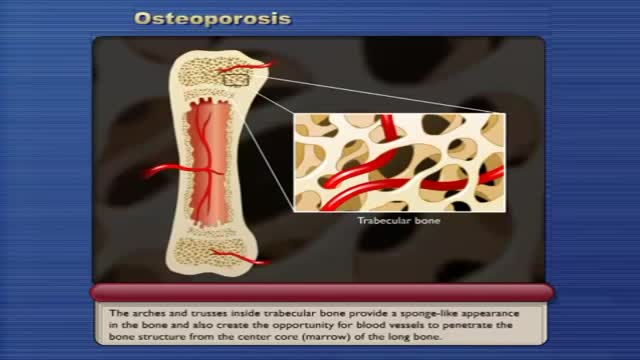
Osteoporosis causes bones to become weak and brittle — so brittle that a fall or even mild stresses such as bending over or coughing can cause a fracture. Osteoporosis-related fractures most commonly occur in the hip, wrist or spine. Bone is living tissue that is constantly being broken down and replaced. Osteoporosis occurs when the creation of new bone doesn't keep up with the removal of old bone. Osteoporosis affects men and women of all races. But white and Asian women — especially older women who are past menopause — are at highest risk. Medications, healthy diet and weight-bearing exercise can help prevent bone loss or strengthen already weak bones.

Spigelian Hernia on Ultrasound

Thinking about laser eye surgery? Watch our live stream and learn what the procedure involves.
Find out more about laser eye surgery
on our website: www.opticalexpress.co.uk
in our online magazine: www.opticalexpress.co.uk/magazine
on our Facebook page: https://www.facebook.com/opticalexpress/
or on our Instagram page: https://www.instagram.com/opticalexpressuk

Bariatric surgical procedures cause weight loss by restricting the amount of food the stomach can hold, causing malabsorption of nutrients, or by a combination of both gastric restriction and malabsorption. Bariatric procedures also often cause hormonal changes. Most weight loss surgeries today are performed using minimally invasive techniques (laparoscopic surgery). The most common bariatric surgery procedures are gastric bypass, sleeve gastrectomy, adjustable gastric band, and biliopancreatic diversion with duodenal switch. Each surgery has its own advantages and disadvantages.

This minimally invasive procedure employs two small cuts rather than a long incision before fusing two vertebra together. The result is less pain, as well as quicker recovery. ~ Detroit Medical Center

Iron is a mineral that plays a vital role in health and well-being. Without it, many bodily functions would malfunction. “The primary role of iron is to carry oxygen in the blood to every cell in the body,” says Beth Thayer, RDN, MS, director of the Center for Health Promotion and Disease Prevention at Henry Ford Health System in Detroit. Iron is an important component of hemoglobin, the protein in red blood cells that carries oxygen from the lungs and transports it throughout the body.
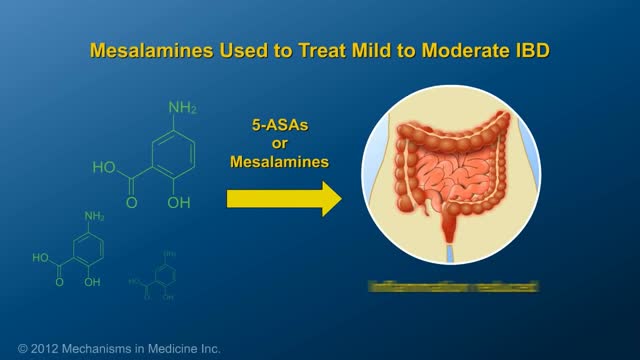
This animation describes risks of inflammatory bowel disease (IBD) and risks/benefits of medication (5-ASAs, steroids, immunomodulators, & biologics).
A detailed animation video explaining a spinal cord injury.
