- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A patient at a British hospital played Mahler and Gershwin on the violin while surgeons removed a tumor from her brain, so doctors could preserve her ability to play music.
She left the hospital 3 days later and hopes to return to the symphony soon. https://abcn.ws/2SGY9mp
SUBSCRIBE to ABC NEWS: https://www.youtube.com/ABCNews/
Watch More on http://abcnews.go.com/
LIKE ABC News on FACEBOOK
https://www.facebook.com/abcnews
FOLLOW ABC News on TWITTER:
https://twitter.com/abc
GOOD MORNING AMERICA'S HOMEPAGE:
https://www.goodmorningamerica.com/

An inguinal hernia occurs when tissue, such as part of the intestine, protrudes through a weak spot in the abdominal muscles. The resulting bulge can be painful, especially when you cough, bend over or lift a heavy object. However, many hernias do not cause pain.
An inguinal hernia isn't necessarily dangerous. It doesn't improve on its own, however, and can lead to life-threatening complications. Your doctor is likely to recommend surgery to fix an inguinal hernia that's painful or enlarging. Inguinal hernia repair is a common surgical procedure.

Circumcision Video 3D

Care must be taken to prevent stenosis at the anastomotic site. If the diameter of the anastomosis is less than 2 cm, the anastomosis should be taken down and resected. A classic end-to-end anastomosis should be performed to ensure adequate diameter to the intestine. If the posterior wall of the colon has been preserved, care should be taken to close the colostomy prior to opening the peritoneal cavity. This will reduce intraperitoneal contamination from the stoma site. Copious irrigation of the wound should be made prior to primary closure. If gross contamination has occurred, delayed closure of the wound should be considered.

OB_A_1013
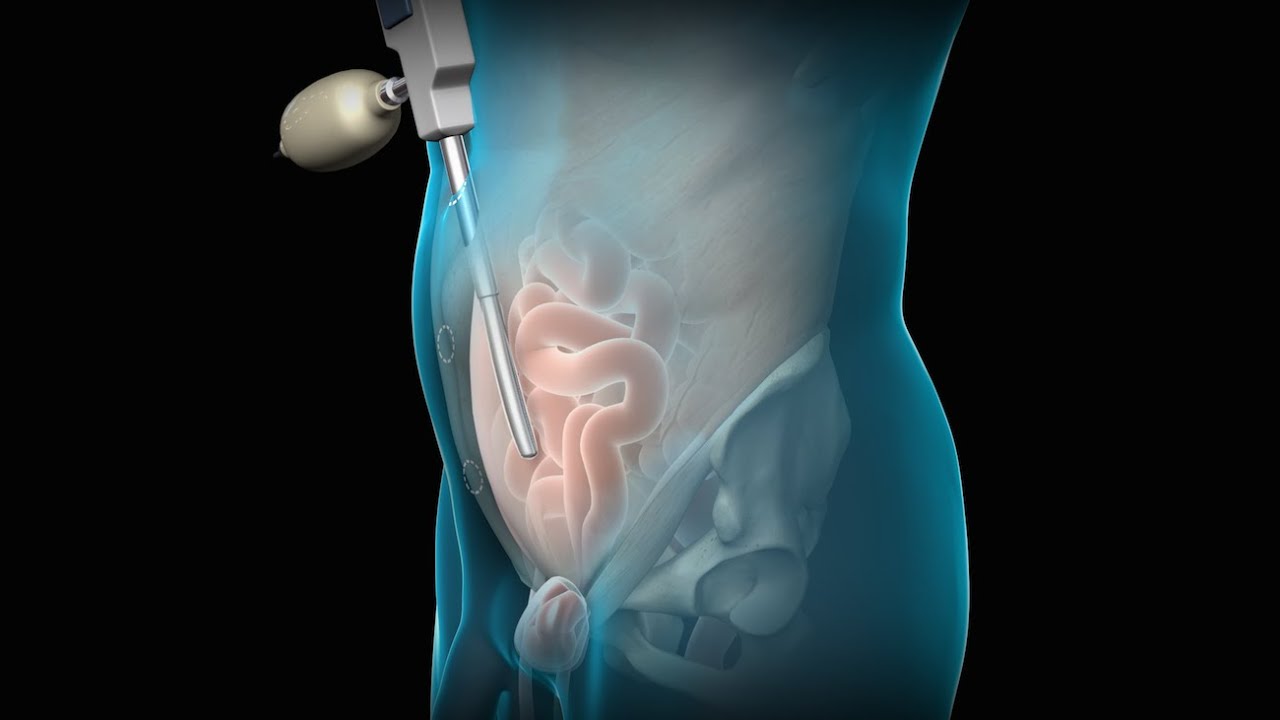
3D animation depicting the operating room and initial procedure preparing the patient for a laparoscopic hysterectomy. The patient is prepped and draped in the usual fashion and surrounded by the surgeon and surgical assistants. The skin is elevated, an infraumbilical incision is made, a trocar port is inserted through the incision and the abdomen is insufflated. Finally, a laparoscope is inserted into the port to allow for direct visualization of the uterus and the surgery can begin.
To view more animations and exhibits, visit our medical library: https://www.trialexhibitsinc.c....om/library/multimedi
Contact us on your next case for consulting, trial graphics, animations, medical illustrations or presentation services. 800-591-1123 [a]www.trialex.com[/a]
This video is for reference only. The video may not be otherwise used, reproduced nor modified. For more information to purchase a copy or permission to use this animation on your next case, project, website or TV, contact us at [a]www.trialex.com[/a] or 800-591-1123.
Copyright @ Trial Exhibits, Inc.
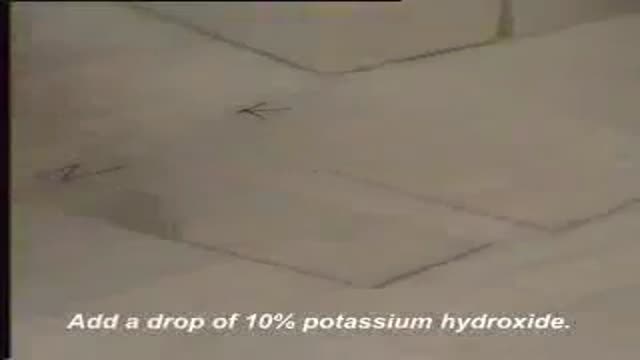
A wet mount is the suspension of a small amount of vaginal discharge in a liquid medium. Two liquids are commonly used, normal saline and potassium hydroxide. Each has it's own unique properties that make it useful in this setting

What is Venipuncture? While venipuncture can refer to a variety of procedures, including the insertion of IV tubes into a vein for the direct application of medicine to the blood stream, in phlebotomy venipuncture refers primarily to using a needle to create a blood evacuation point. As a phlebotomist, you must be prepared to perform venipuncture procedures on adults, children, and even infants while maintaining a supportive demeanor and procedural accuracy. Using a variety of blood extraction tools, you must be prepared to respond to numerous complications in order to minimize the risk to the patient while still drawing a clean sample. In its entirety, venipuncture includes every step in a blood draw procedure—from patient identification to puncturing the vein to labeling the sample. Patient information, needle placement, and emotional environment all play a part in the collection of a blood sample, and it's the fine details that can mean the difference between a definite result and a false positive. After placing the tourniquet and finding the vein, it's time for the phlebotomist to make the complex choice on what procedure will best suit the specific situation. Keeping this in mind, it should be noted that the following information is not an instructional guide on how to perform these phlebotomy procedures. Rather, the information below is intended to serve as an educational resource to inform you of the equipment and procedures you will use. Venipuncture Technqiues Venipuncture with an Evacuated or Vacuum Tube: This is the standard procedure for venipuncture testing. Using a needle and sheath system, this procedure allows multiple sample tubes to be filled through a single puncture. This procedure is ideal for reducing trauma to patients. After drawing the blood, the phlebotomist must make sure the test stopper is correctly coded and doesn't contact exposed blood between samples. Venipuncture with a Butterfly Needle : This is a specialized procedure that utilizes a flexible, butterfly needle adaptor. A butterfly needle has two plastic wings (one on either side of the needle) and is connected to a flexible tube, which is then attached to a reservoir for the blood. Due to the small gauge of the needle and the flexibility of the tube, this procedure is used most often in pediatric care, where the patients tend to have smaller veins and are more likely to move around during the procedure. After being inserted into a vein at a shallow angle, the butterfly needle is held in place by the wings, which allow the phlebotomist to grasp the needle very close to the skin. Phlebotomists should be careful to watch for blood clots in the flexible tubing. Venipuncture with a Syringe: This technique is typically only used when there is a supply shortage, or when a technician thinks it is the appropriate method. It uses the classic needle, tube, and plunger system, operating in a similar manner to the vacuum tube but requiring multiple punctures for multiple samples. Additionally, after the blood is drawn it must be transferred to the appropriate vacuum tube for testing purposes. If you choose to use this method, remember to check for a sterile seal, and use a safety device when transferring the sample. Fingerstick (or Fingerprick): This procedure uses a medical lance to make a small incision in the upper capillaries of a patient's finger in order to collect a tiny blood sample. It is typically used to test glucose and insulin levels. When performing a Fingerstick, the phlebotomist should remember to lance the third or fourth finger on the non-dominant arm. Never lance the tip or the center of the finger pad; instead, lance perpendicular to the fingerprint lines. Heelstick (or Heelprick): Similar to the Fingerstick procedure, this process is used on infants under six months of age. A medical lance is used to create a small incision on the side of an infant's heel in order to collect small amounts of blood for screening. As with a Fingerstick, the incision should be made perpendicular to the heel lines, and it should be made far enough to the left or right side of the heel to avoid patient agitation. Before performing a Heelstick, the infant's heel should be warmed to about 42 degrees Celsius in order to stimulate capillary blood and gas flow. Therapeutic Phlebotomy: This involves the actual letting of blood in order to relieve chemical and pressure imbalances within the blood stream. Making use of a butterfly needle, this therapy provides a slow removal of up to one pint of blood. Though the blood removed is not used for blood transfusions, the procedure and concerns are the same as with routine blood donation. As with any phlebotomy procedure, one should pay close attention to the patient in order to prevent a blood overdraw. Bleeding Time: A simple diagnostic test that is used to determine abnormalities in blood clotting and platelet production. A shallow laceration is made, followed by sterile swabbing of the wound every 30 seconds until the bleeding stops. Average bleed times range between one and nine minutes. As a phlebotomist, you should familiarize yourself with the application and cross-application of these procedures in order to recognize when a procedure is necessary, and what the risks are for each.

German Video showing examination of the urinary bladder
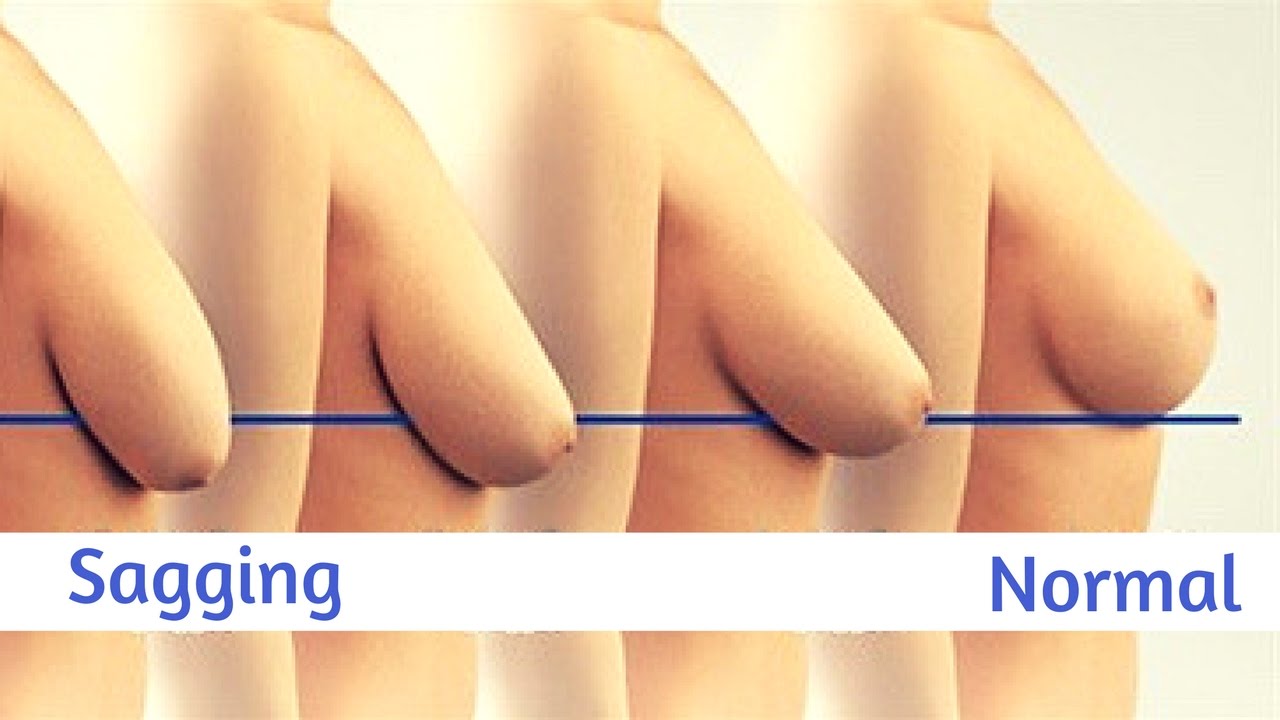
Watch that video to know How To Firm And Lift Your Sagging Breasts Naturally

Dr. Joseph McGinn explains minimally invasive bypass, the procedure he pioneered as an alternative to open heart surgery.

Butt implants are a popular plastic surgery procedure among those who wish to enhance the appearance, shape, and size of their rear ends. Buttock augmentation involves the surgical insertion of artificial body implants into a patient’s buttocks to create a larger, shapelier, and more sensuous rear end. Patients who have underdeveloped buttocks can achieve a more proportionate figure with butt implants. Women who wish to achieve an “hour glass” figure or are unhappy with the size of their buttocks can benefit from female butt implants. Men with flat or poorly developed buttocks can enhance the shape of the area to their liking with male butt implants. Many buttock augmentation patients say that their clothes fit better, they feel more attractive, and their confidence levels have improved.
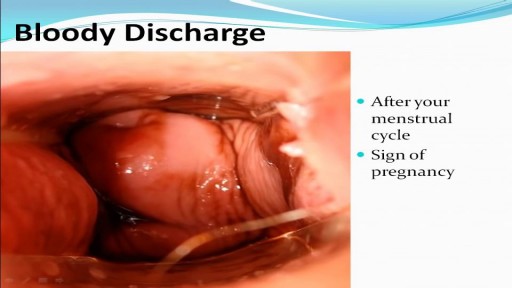
Watch that video to know the Types of Female Genital discharge

Demonstrates some of the procedures of the Cardio Vascular / Peripheral Vascular exam.

Orchidectomy and Orchidopexy in Testicular Torsion
To license this video for patient education or content marketing, visit: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=tephernia-030615
An inguinal hernia is a bulging of the intestine through a defect or weak spot in the wall of the lower abdomen. This video shows how inguinal hernias form and how they are treated.
#TotalExtraperitonealLaparoscopicInguinalHerniaRepair #TEP #laparoscopy
ANCE00200

Intrauterine insemination (IUI) is a fertility treatment that involves placing sperm inside a woman's uterus to facilitate fertilization. The goal of IUI is to increase the number of sperm that reach the fallopian tubes and subsequently increase the chance of fertilization


This video shows the delivery of the placenta after delivery of the fetus

Female to Male gender confirming top surgery video : "Double Incision" Technique.

Hardware removals are among the most commonly performed surgical procedures worldwide. Current literature offers little data concerning postoperative patient satisfaction. The purpose of our study was to evaluate the patients’ point of view on implant removal. watch to learn more.
