- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Treatment of bowel injury by IUD

Initial symptoms may include: Pain or discomfort in the upper tummy (abdomen), especially after eating. Indigestion. (Note: most people who have indigestion do not have stomach cancer.) Feeling sick, and being off food. ... Weight loss and/or loss of appetite. You may pass blood out with your stools (faeces).
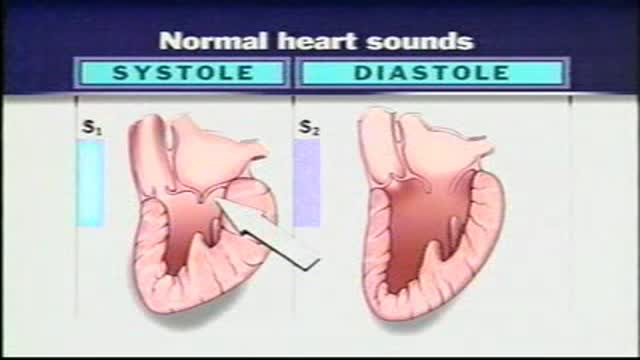
Normal Heart Sounds With the aid of a stethoscope you can hear the characteristic sounds of the normal heartbeat, typically described as a "lub-dub." These sounds are produced by the closure of the heart valves. The first heart sound or "lub" results from closure of the tricuspid and mitral valves. It is a rather low-pitched and a relatively long sound which, as indicated in, represents the beginning of ventricular systole. The second heart sound, or "dub," marks the beginning of ventricular diastole. It is produced by closure of the aortic and pulmonary (pulmonic) semilunar vanes when the intraventricular pressure begins to fall. This "dub" sound is typically heard as a sharp snap because the semilunar valves tend to close much more rapidly than the AV valves. Because diastole occupies more time than systole, a brief pause occurs after the second heart sound when the heart is beating at a normal rate. Therefore, the pattern that one hears is one of: "lub-dub" pause, "lub-dub" pause, and so on. Sometimes, especially in young normal individuals, a third heart sound can be heard. This sound is produced by the very rapid influx of blood into the partially filled ventricle. It is typically very faint and as such difficult to hear.
Gleevecs mechanism of Action

General Considerations Because a discussion of reproductive issues may be difficult for some women, it is important to obtain the history in a relaxed and private setting. The patient should be clothed, particularly if she is meeting the provider for the first time. Ordinarily, the patient should be interviewed alone. Exceptions may be made for children, adolescents, and mentally impaired women, or if the patient specifically requests the presence of a caretaker, friend, or family member. However, even in these circumstances, it is desirable for the patient to have some time to speak with the clinician privately. The manner of address should be formal using the title Mrs., Ms., Miss, or Dr. with the patient’s surname, unless the patient requests otherwise. In some settings, it may be appropriate for nursing staff to be involved with history taking. A nurse may be perceived as less threatening, and may be able to take the history in a less hurried manner.1 The provider can verify the history and focus on areas of concern. Alternatively, it may be helpful to ask the patient to complete a self-history form on paper or by computer prior to speaking with the provider. This allows the provider to devote time to addressing positive responses, and ensures that important questions are not missed. Hasley2 showed that responses to a computer-based questionnaire designed to update a patient’s gynecologic history were equivalent to those obtained during a personal interview. Several studies involving patients in non-gynecologic settings have shown that patients are more likely to provide sensitive information when responding to a computer-based questionnaire as opposed to a personal interview or even a paper questionnaire.3 In order to increase a patient’s level of comfort during the interview, questions should be asked in an open-ended and nonjudgmental way. Assumptions should not be made about aspects of the patient’s background such as sexual orientation. At the conclusion of the interview, patients should be asked whether there are concerns that they would like to discuss that were not addressed previously in the interview.

Meet Christian, an incredible man born with no arms or legs who lives life to the fullest
This minimally invasive procedure connects electrodes to the brain and places a pacemaker-like device under the skin. When activated, electrical impulses minimize shaking due to "dyskinesia syndrome" in patients with Parkinson's disease. ~ Detroit Medical Center

Ventricular fibrillation is a heart rhythm problem that occurs when the heart beats with rapid, erratic electrical impulses. This causes pumping chambers in your heart (the ventricles) to quiver uselessly, instead of pumping blood. Sometimes triggered by a heart attack, ventricular fibrillation causes your blood pressure to plummet, cutting off blood supply to your vital organs. Ventricular fibrillation, an emergency that requires immediate medical attention, causes the person to collapse within seconds. It's the most frequent cause of sudden cardiac death. Emergency treatment includes cardiopulmonary resuscitation (CPR) and shocks to the heart with a device called a defibrillator. Treatments for those at risk of ventricular fibrillation include medications and implantable devices that can restore a normal heart rhythm.

This minimally invasive procedure employs two small cuts rather than a long incision before fusing two vertebra together. The result is less pain, as well as quicker recovery. ~ Detroit Medical Center

Epley maneuver: Step 1 You will sit on the doctor's exam table with your legs extended in front of you. The doctor will turn your head so that it is halfway between looking straight ahead and looking directly to the side that causes the worst vertigo. Without changing your head position, the doctor will guide you back quickly so that your shoulders are on the table but your head is hanging over the edge of the table. In this position, the side of your head that is causing the worst vertigo is facing the floor. The doctor will hold you in this position for 30 seconds or until your vertigo stops. Epley maneuver: Step 2 Then, without lifting up your head, the doctor will turn your head to look at the same angle to the opposite side, so that the other side of your head is now facing the floor. The doctor will hold you in this position for 30 seconds or until your vertigo stops. Epley maneuver: Step 3 The doctor will help you roll in the same direction you are facing so that you are now lying on your side. (For example, if you are looking to your right, you will roll onto your right side.) The side that causes the worst vertigo should be facing up. The doctor will hold you in this position for another 30 seconds or until your vertigo stops. Epley maneuver: Step 4 The doctor will then help you to sit back up with your legs hanging off the table on the same side that you were facing. This maneuver is done with the assistance of a doctor or physical therapist. A single 10- to 15-minute session usually is all that is needed. When your head is firmly moved into different positions, the crystal debris (canaliths) causing vertigo will move freely and no longer cause symptoms.

DMC Specialists use minimally invasive surgery to remove an extremely large uterine fibroid from a patient. ~ Detroit Medical Center

Thinking about laser eye surgery? Watch our live stream and learn what the procedure involves.
Find out more about laser eye surgery
on our website: www.opticalexpress.co.uk
in our online magazine: www.opticalexpress.co.uk/magazine
on our Facebook page: https://www.facebook.com/opticalexpress/
or on our Instagram page: https://www.instagram.com/opticalexpressuk
Interventional Nephrology is a new and emerging subspecialty of Nephrology that mainly deals with ultrasonography of kidneys and ultrasound-guided renal biopsy, insertion of peritoneal dialysis catheters, tunneled dialysis catheters as a vascular access for patients undergoing hemodialysis as well as percutaneous ...
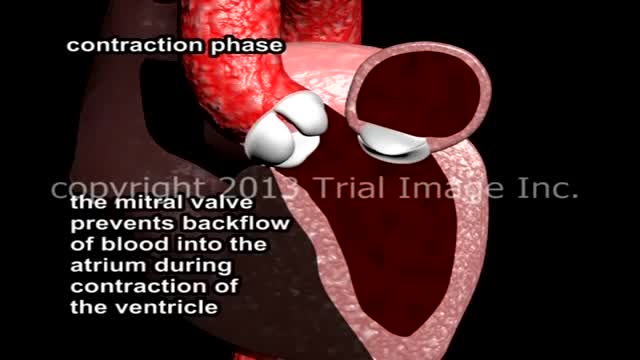
Mitral Valve Prolapse and Mitral Regurgitation. Review of mitral valve anatomy and function, including papillary muscle structure and function, with severe mitral valve prolapse and mitral regurgitation due to a flail segment caused by ruptured papillary muscle and chorda tendinae attachment.

Stephen has got the medical treatment at Asian Hip Resurfacing Surgical Center in india.
Dr.Vijay Bose (Orthopedic Consultant),
Asian Hip Resurfacing Surgical Center.
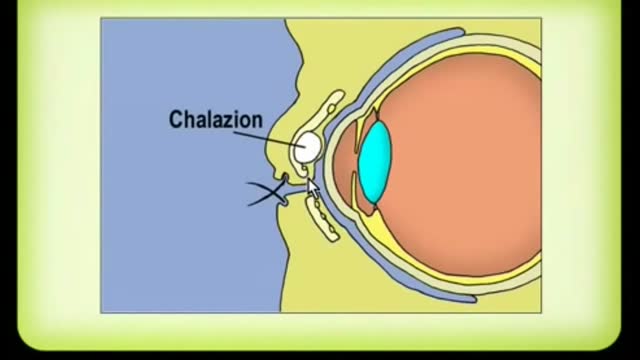
A chalazion is a lump of the lid that is caused by obstruction of the drainage duct of an oil gland within the upper or lower eyelid. This lump may increase in size over days to weeks and may occasionally become red, warm, or painful.

Acute intermittent porphyria (AIP) is a rare autosomal dominant metabolic disorder affecting the production of heme, the oxygen-binding prosthetic group of hemoglobin. It is characterized by a deficiency of the enzyme porphobilinogen deaminase.
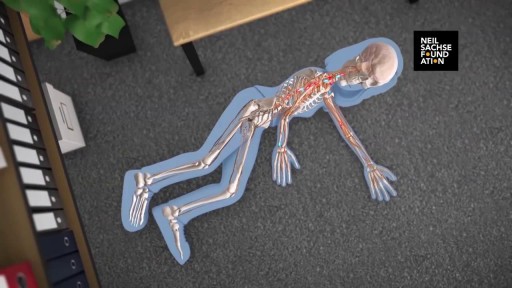
A detailed animation video explaining a spinal cord injury.

An antecedent upper respiratory infection is present in 50% of patients. Abdominal pain is a presenting symptom in 1 0-15% of patients. The skin lesions are symmetric, involve dependent parts of the body, and classically progress from an erythematous, macular rash to papular purpura. The joints and kidneys are also commonly involved

Device that keeps a donor heart beating
