- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
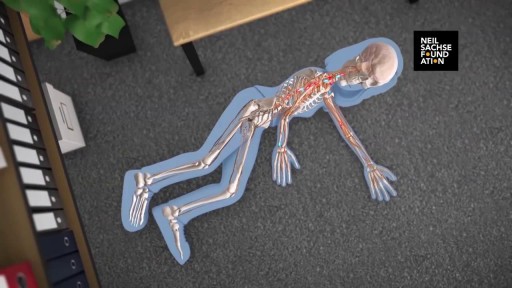
A detailed animation video explaining a spinal cord injury.
How to Reverse GERD and Leaky Gut

The ABC's of Adult CPR
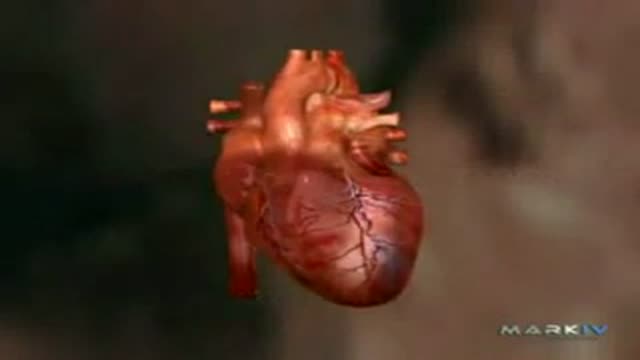
Acute Myocardial Infarction - Heart Attack

Angioplasty Procedure Animation
Wash your hands thoroughly with soap and water before and after treating the wound. Wash the area with mild soap and running water to reduce the risk of infection. Pat dry. Apply antibiotic ointment and cover with a clean bandage or sterile dressing. Antibiotic prophylaxis should be considered, especially if there is a high risk of infection, such as with cat bites, with puncture wounds, with wounds to the hand, and in persons who are immunosuppressed. Amoxicillin/clavulanate is the first-line prophylactic antibiotic.
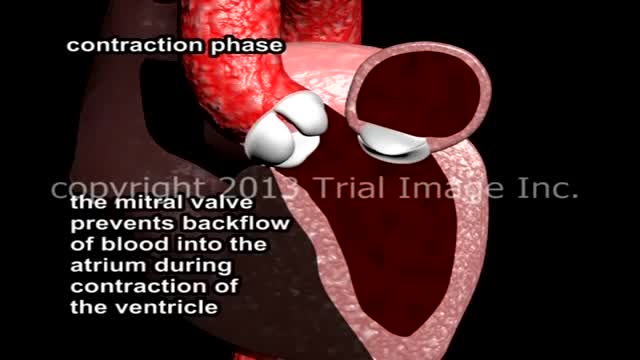
Mitral Valve Prolapse and Mitral Regurgitation. Review of mitral valve anatomy and function, including papillary muscle structure and function, with severe mitral valve prolapse and mitral regurgitation due to a flail segment caused by ruptured papillary muscle and chorda tendinae attachment.

This minimally invasive procedure employs two small cuts rather than a long incision before fusing two vertebra together. The result is less pain, as well as quicker recovery. ~ Detroit Medical Center

Next to esophagojejunostomy stapling for the reconstruction following total gastrectomy, several silk stitches anchoring the jejunum to endoabdominal fascia are made to restore the function of phrenoesophageal ligament.
anchoring suture reduces the impairment of the anastomotic blood flow that is caused by gravitational tension and so is useful to protect the esophagojejunostomy after total gastrectomy.
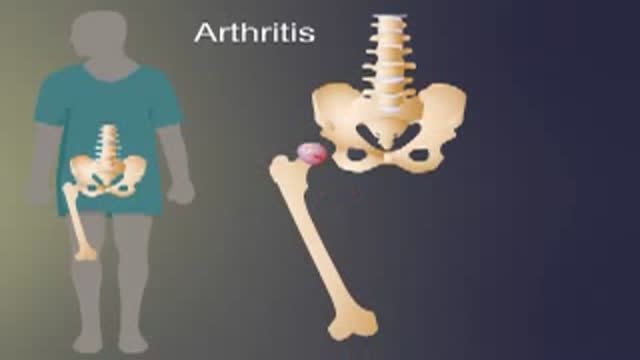
Arthritis of the hip causes severe pain, and sometimes requires surgical treatment, including hip replacement. This animated video show you what hip arthritis is, and how it causes symptoms.
The maneuver is commonly used during some activities: Straining to have a bowel movement Blowing a stuffy nose Certain medical tests or exams As a pressure equalization technique by scuba divers, sky divers and airplane passengers The effect of the Valsalva Maneuver is a drastic increase in the pressure within the thoracic cavity.

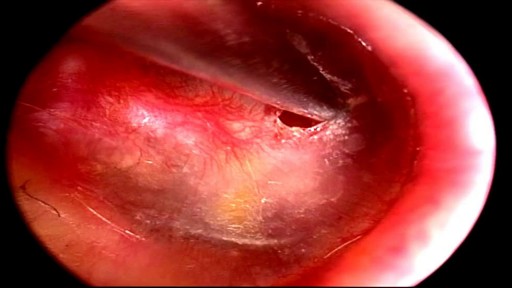
Tonsillitis is inflammation of the tonsils, two oval-shaped pads of tissue at the back of the throat — one tonsil on each side. Signs and symptoms of tonsillitis include swollen tonsils, sore throat, difficulty swallowing and tender lymph nodes on the sides of the neck. Most cases of tonsillitis are caused by infection with a common virus, but bacterial infections also may cause tonsillitis. Because appropriate treatment for tonsillitis depends on the cause, it's important to get a prompt and accurate diagnosis. Surgery to remove tonsils, once a common procedure to treat tonsillitis, is usually performed only when bacterial tonsillitis occurs frequently, doesn't respond to other treatments or causes serious complications.

Conduct disorder (CD) is a mental disorder diagnosed in childhood or adolescence that presents itself through a repetitive and persistent pattern of behavior in which the basic rights of others or major age-appropriate norms are violated. These behaviors are often referred to as "antisocial behaviors."

Ventricular fibrillation is a heart rhythm problem that occurs when the heart beats with rapid, erratic electrical impulses. This causes pumping chambers in your heart (the ventricles) to quiver uselessly, instead of pumping blood. Sometimes triggered by a heart attack, ventricular fibrillation causes your blood pressure to plummet, cutting off blood supply to your vital organs. Ventricular fibrillation, an emergency that requires immediate medical attention, causes the person to collapse within seconds. It's the most frequent cause of sudden cardiac death. Emergency treatment includes cardiopulmonary resuscitation (CPR) and shocks to the heart with a device called a defibrillator. Treatments for those at risk of ventricular fibrillation include medications and implantable devices that can restore a normal heart rhythm.

Treatment of bowel injury by IUD
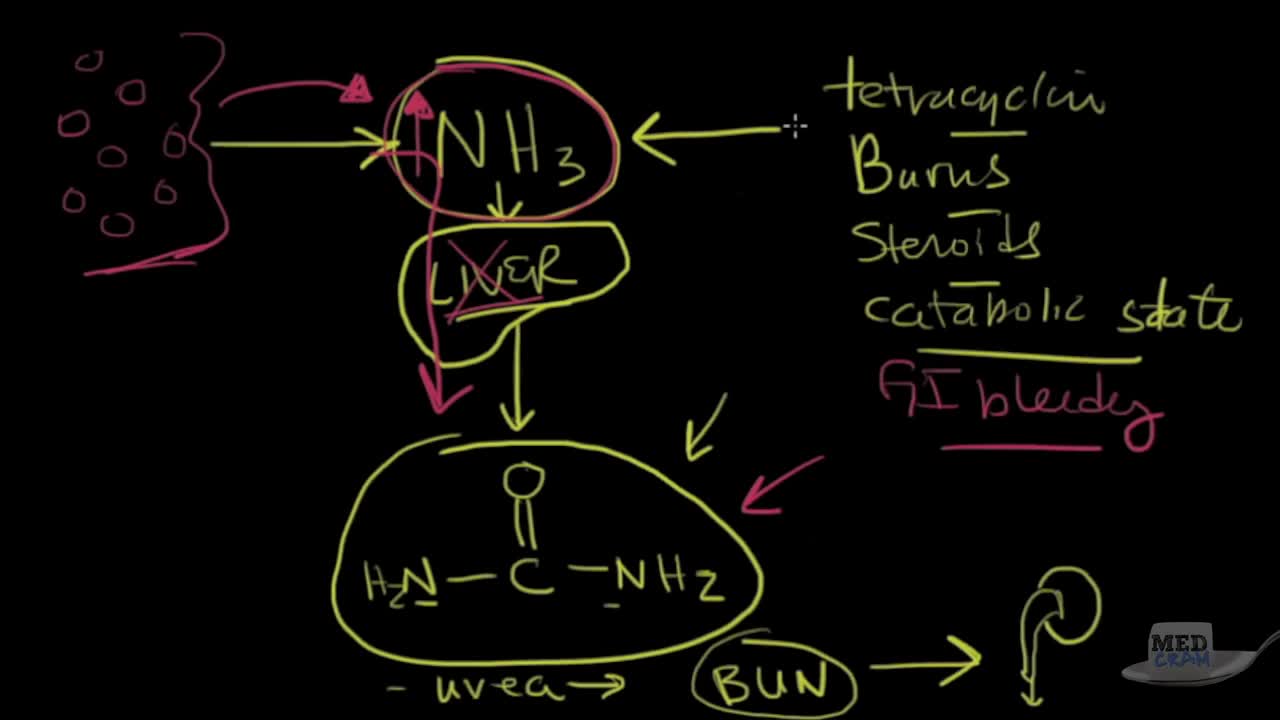
Acute kidney failure — also called acute renal failure or acute kidney injury — develops rapidly over a few hours or a few days. Acute kidney failure is most common in people who are already hospitalized, particularly in critically ill people who need intensive care. Acute kidney failure can be fatal and requires intensive treatment. However, acute kidney failure may be reversible. If you're otherwise in good health, you may recover normal or nearly normal kidney function
This minimally invasive procedure connects electrodes to the brain and places a pacemaker-like device under the skin. When activated, electrical impulses minimize shaking due to "dyskinesia syndrome" in patients with Parkinson's disease. ~ Detroit Medical Center

very funny medical video..DO NOT TRY AT CLINIC
