- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Liver transplantation is surgery to remove a diseased or injured liver and replace it with a healthy whole liver or a segment of a liver from another person, called a donor. People with either acute or chronic liver failure may need a liver transplant to survive.

Cerebral palsy is a disorder of movement, muscle tone or posture that is caused by damage that occurs to the immature, developing brain, most often before birth. Signs and symptoms appear during infancy or preschool years. In general, cerebral palsy causes impaired movement associated with abnormal reflexes, floppiness or rigidity of the limbs and trunk, abnormal posture, involuntary movements, unsteady walking, or some combination of these. People with cerebral palsy may have problems swallowing and commonly have eye muscle imbalance, in which the eyes don't focus on the same object. People with cerebral palsy also may suffer reduced range of motion at various joints of their bodies due to muscle stiffness. Cerebral palsy's effect on functional abilities varies greatly. Some affected people can walk while others can't. Some people show normal or near-normal intellectual capacity, but others may have intellectual disabilities. Epilepsy, blindness or deafness also may be present.
Absence of a woman's monthly menstrual period is called amenorrhea. Secondary amenorrhea is when a woman who has been having normal menstrual cycles stops getting her periods for 6 months or longer. Causes Secondary amenorrhea can occur due to natural changes in the body. For example, the most common cause of secondary amenorrhea is pregnancy. Breastfeeding and menopause are also common, but natural, causes. Women who take birth control pills or who receive hormone shots such as Depo-Provera may not have any monthly bleeding. When they stop taking these hormones, their periods may not return for more than 6 months. You are more likely to have absent periods if you: Are obese Exercise too much and for long periods of time Have very low body fat (less than 15 to 17%) Have severe anxiety or emotional distress Lose a lot of weight suddenly (for example, from strict or extreme diets or after gastric bypass surgery) Other causes include: Brain (pituitary) tumors Drugs for cancer treatment Drugs to treat schizophrenia or psychosis Overactive thyroid gland Polycystic ovarian syndrome Reduced function of the ovaries
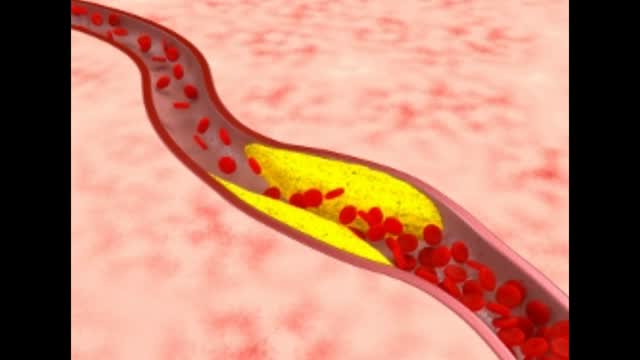
This video: Claudication is pain caused by too little blood flow, usually during exercise. Sometimes called intermittent claudication, this condition generally affects the blood vessels in the legs, but claudication can affect the arms, too. At first, you'll probably notice the pain only when you're exercising, but as claudication worsens, the pain may affect you even when you're at rest. Although it's sometimes considered a disease, claudication is technically a symptom of a disease. Most often, claudication is a symptom of peripheral artery disease, a potentially serious but treatable circulation problem in which the vessels that supply blood flow to your legs or arms are narrowed. Fortunately, with treatment, you may be able to maintain an active lifestyle without pain.
Alzheimer’s disease is the most common cause of dementia and also the best understood. It is thought to be caused by the formation of abnormal deposits of protein in the brain.
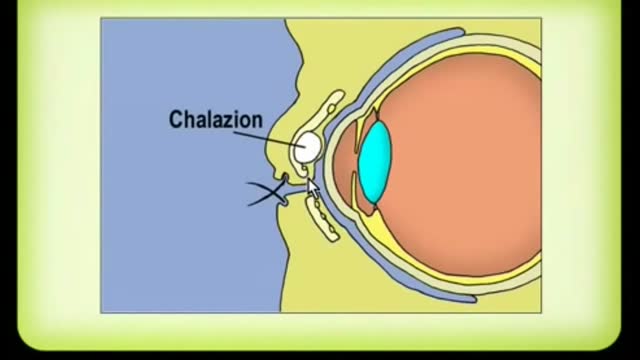
A chalazion is a lump of the lid that is caused by obstruction of the drainage duct of an oil gland within the upper or lower eyelid. This lump may increase in size over days to weeks and may occasionally become red, warm, or painful.

New flu vaccines are released every year to keep up with rapidly adapting flu viruses. Because flu viruses evolve so quickly, last year's vaccine may not protect you from this year's viruses. After vaccination, your immune system produces antibodies that will protect you from the vaccine viruses.

A man's age matters. As men get older, the chances of conceiving and having a healthy child decline. Male fertility starts to decline after 40 when sperm quality decreases. This means it takes longer for their partners to conceive and when they do, there's an increased risk of miscarriage.

Insert the needle into the rubber stopper of the insulin bottle. Push the plunger down to inject air into the bottle (this allows the insulin to be drawn more easily). Leave the needle in the bottle. Turn the bottle and syringe upside-down.
How to Check Cervical Mucus

Dehydration can also be a cause of kidney stones. A common symptom is having a lower left abdominal pain, fever, nausea, groin pain and vomiting. Lower left abdominal pain can also be caused by an infection of the kidneys. It usually begins with the bladder and then reaches out to the kidneys.

Unbelievable Bladder Stone Removal
Non-Hodgkin's lymphoma, also called non-Hodgkin lymphoma, is cancer that originates in your lymphatic system, the disease-fighting network spread throughout your body. In non-Hodgkin's lymphoma, tumors develop from lymphocytes — a type of white blood cell. Non-Hodgkin's lymphoma is more common than the other general type of lymphoma — Hodgkin lymphoma. Many different subtypes of non-Hodgkin's lymphoma exist. The most common non-Hodgkin's lymphoma subtypes include diffuse large B-cell lymphoma and follicular lymphoma.
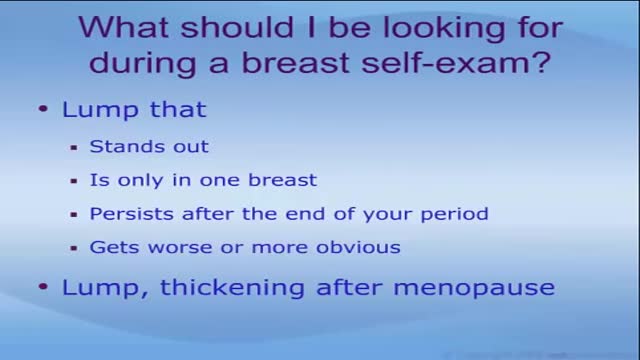
Breast lumps facts Breast lumps can be caused by infections, injuries, non-cancerous growths, and cancer. Breast cancer usually causes no pain in the breast. The symptoms of breast cancer include painless breast lumps, nipple discharge, and inflammation of the skin of the breast. The chances that a particular breast lump could be cancerous depends on many factors, including past medical history, physical examination, as well as genetic and other risk factors. The only way to be certain that a lump is not cancerous is to have a tissue sampling (biopsy). There are several ways to do the biopsy. The treatment of a breast lump depends on its cause.

Controlled studies on treatment of catscratch disease (CSD) are lacking. Thus, treatment recommendations are based on case reports, reviews, a single controlled trial, and anecdotal data. Practice guidelines for the diagnosis and management of skin and soft-tissue infections, including CSD, have been established.Oct 19, 2016

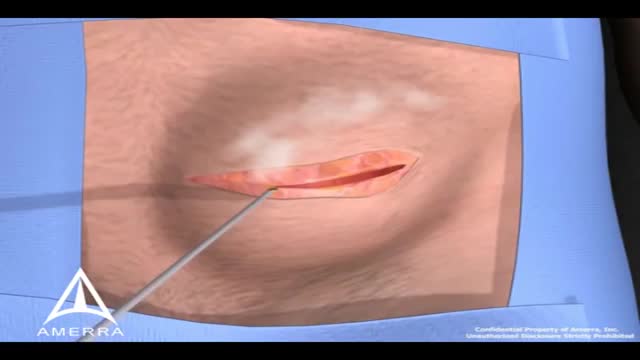
Breast abscesses are often linked to mastitis – a condition that causes breast pain and swelling (inflammation), and usually affects women who are breastfeeding. Infections can occur during breastfeeding if bacteria enter your breast tissue, or if the milk ducts (tiny tubes) become blocked. This can cause mastitis which, if not treated, can result in an abscess forming. Women who aren't breastfeeding can also develop mastitis if bacteria enter the milk ducts through a sore or cracked nipple, or a nipple piercing. White blood cells are sent to attack the infection, which causes tissue at the site of the infection to die. This creates a small, hollow area that fills with pus (an abscess).
During surgery to repair the hernia, the bulging tissue is pushed back in. Your abdominal wall is strengthened and supported with sutures (stitches), and sometimes mesh. This repair can be done with open or laparoscopic surgery. You and your surgeon can discuss which type of surgery is right for you.
Root canals are common procedures and can help save your tooth from extraction. Dentists at Aspen Dental practices have been safely and expertly performing root canal procedures for over two decades.

One technique to relocate a dislocated elbow with anatomy diagrammed out.

Colonoscopy is a test that allows your doctor to look at the inner lining of your large intestine (rectum and colon). He or she uses a thin, flexible tube called a colonoscope to look at the colon. A colonoscopy helps find ulcers, colon polyps, tumors, and areas of inflammation or bleeding.
