- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
The goal of COPD management is to improve a patient’s functional status and quality of life by preserving optimal lung function, improving symptoms, and preventing the recurrence of exacerbations. Currently, no treatments aside from lung transplantation have been shown to significantly improve lung function or decrease mortality; however, oxygen therapy (when appropriate) and smoking cessation may reduce mortality. Once the diagnosis of COPD is established, it is important to educate the patient about the disease and to encourage his or her active participation in therapy.
Patent ductus arteriosus (PDA), in which there is a persistent communication between the descending thoracic aorta and the pulmonary artery that results from failure of normal physiologic closure of the fetal ductus (see image below), is one of the more common congenital heart defects.

If you could stand in someone else's shoes...Hear what they hear See what they see Feel what they fell Would you treat them differently?
Epilepsy is the fourth most common neurological disorder and affects people of all ages Epilepsy means the same thing as "seizure disorders" Epilepsy is characterized by unpredictable seizures and can cause other health problems Epilepsy is a spectrum condition with a wide range of seizure types and control varying from person-to-person Public perception and misunderstanding of epilepsy causes challenges often worse than the seizures

Aparthroereisis

Unbelievable Bladder Stone Removal

Throughout your life, your skin will change constantly, for better or worse. In fact, your skin will regenerate itself approximately every 27 days. Proper skin care is essential to maintaining the health and vitality of this protective organ.

Watch that video to know What is Female G Spot?

Skin Whitening in Delhi ! Skin Lightening By Best Dermatologist in Delhi

Symptoms Of Anxiety, Anxiety Disorder Symptoms, What Is Social Anxiety, Zoloft For Anxiety --- http://panic-attacks-anxiety.good-info.co --- Panic attacks and anxiety While there are times for doctors, I want you to consider this: MOST of your anxiety is under the radar… Masquerading as “just feeling a bit nervous”... or “just a tad irritable thanks to this diet plan”... or, “let’s skip the party and just stay home tonight.” And, I’m telling you, that anxiety not only destroys your fat burning power: It often leads to all-out panic disorder, if you just ignore it. Fortunately for you, there’s a 60-Second Solution that restores your calm, removes those anxious feelings, and allows you to keep burning body fat for energy. Now, this exact same technique works for all-out panic and even more serious anxiety issues, too… The man who delivers this presentation had panic attacks in “everyday” situations… and he too had feelings of anxiety whenever he tried to diet-off body fat… This Simple Trick Stops Panic Attacks And Anxiety Click Here: http://panic-attacks-anxiety.good-info.co

This is an introduction into mole removal through excisional means (cutting it out) or using a laser to remove the mole

our dentist says it's time to remove your wisdom teeth. He may refer you to an oral surgeon, who will do the procedure in his office. It should only take a few days for you to heal and feel back to normal.

Though you might think of your spinal cord as one single piece, it's actually a column of nerves protected by a sheath of myelin and then further secured by 31 butterfly-shaped vertebrae (singular: vertebra). Medical providers divide the spinal cord into four distinct regions. Knowing the region in which the injury is located is often the key to understanding diagnosis and treatment. The four spinal cord regions are: The cervical spinal cord: This is the topmost portion of the spinal cord, where the brain connects to the spinal cord, and the neck connects to the back. This region consists of eight vertebrae, commonly referred to as C1-C8. All spinal cord numbers are descending, so C1 is the highest vertebra, while C8 is the lowest in this region. The thoracic spinal cord: This section forms the middle of the spinal cord, containing twelve vertebrae numbered T1-T12.

Most people develop several moles (nevi) throughout adulthood. Moles can be found anywhere on the body, usually in sun-exposed areas, and are usually brown, smooth, and slightly raised. In most cases, a nevus is benign and doesn't require treatment. Rarely, they turn into melanoma or other skin cancers. A nevus that changes shape, grows bigger, or darkens should be evaluated for removal.


#dialysis #hemodialysis #kidneys
Follow us: https://www.instagram.com/7activestudio/
For more information:
www.7activestudio.com
7activestudio@gmail.com
Contact: +91- 9700061777, 040-66564777
7 Active Technology Solutions Pvt.Ltd. is an educational 3D digital content provider for K-12. We also customise the content as per your requirement for companies platform providers colleges etc . 7 Active driving force "The Joy of Happy Learning" -- is what makes difference from other digital content providers. We consider Student needs, Lecturer needs and College needs in designing the 3D & 2D Animated Video Lectures. We are carrying a huge 3D Digital Library ready to use.
Voice Over Credit: Muls N Ravs Entertainment Pvt. Ltd. (www.mulsnravs.com)


This cancer development medical video is devoted to elaborating the basics of cancer growth. We used advanced medical animation techniques to display such a complicated process.
What is happening in cancer development medical video
The fundamental abnormality described in the cancer development medical video is the nonstop unregulated multiplication of cancer cells. Being uncontrollable by body’s signals that regulate normal cell behavior; cancerous cells divide and grow populating neighboring normal tissues or even spread throughout the body. The overall lack of growth control acquired by cancer cells is due to the accumulated abnormalities in numerous cell regulatory mechanisms and is considered in some aspects of cell behavior that differs them from their healthy counterparts. The interaction of these cells is shown in our previous medical animation video.
Read full article on our webpage http://bit.ly/2LQj9ln
Follow us on Facebook https://www.facebook.com/Nanob....ot.Medical.Animation
Follow us on LinkedIn https://www.linkedin.com/compa....ny/nanobotmodels-med
Follow us on Twitter https://twitter.com/Nanobot_Studio
Follow us on Instagram https://www.instagram.com/nano....bot_medical_animatio
Follow us on Clutch https://clutch.co/profile/nano....bot-medical-animatio
Follow us on Behance https://www.behance.net/NanobotStudio
#cancer #tumor #oncology #metatastic #nanobot #visualscience #scientificcommunication #medicalanimation #animationvideo #animationdesign #animationstudio #animationmovie #nanotechnology #medicine #health #science #education #medschool #medicaleducation #animation_studio #animationstudio
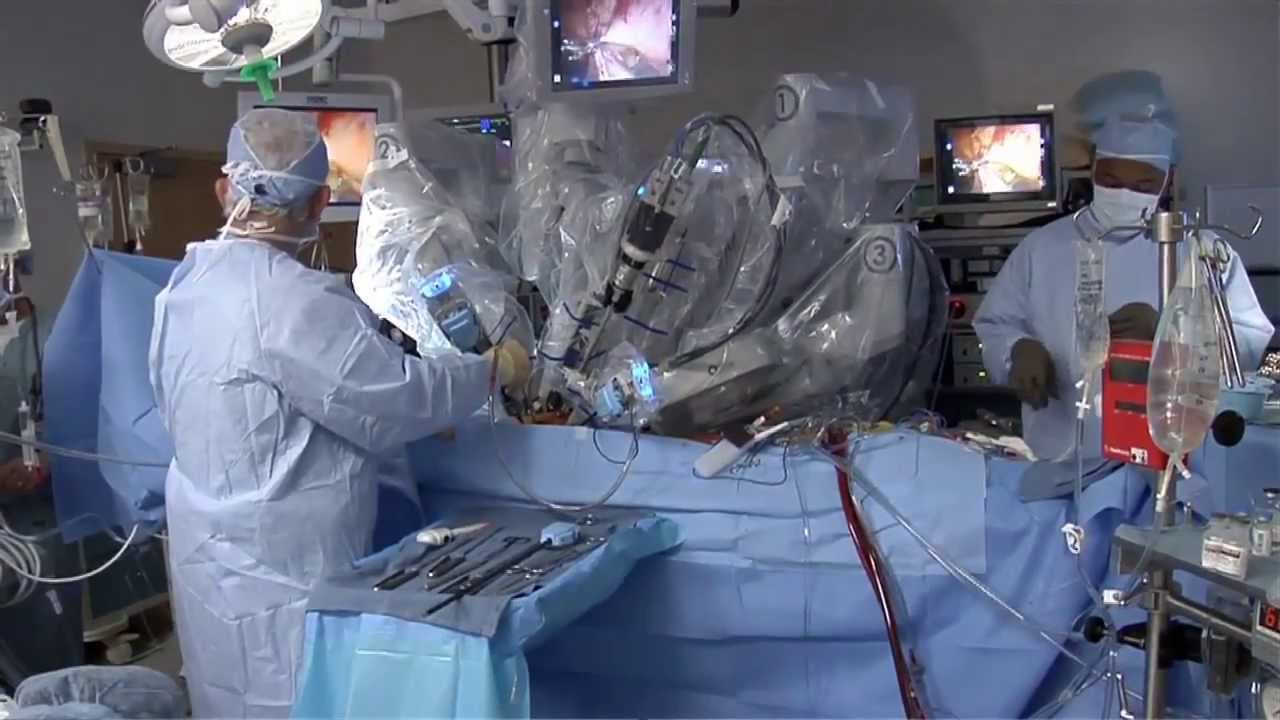
They are the leaders of the pack when it comes to minimally invasive surgeries. Laparoscopic and robotic. Different techniques with the same benefits.
"There's significantly less blood loss, it's a quicker procedure, quicker recovery, less scarring, less chance for post operative wound complications or infections," says Dr. Darren Miter, laparoscopic surgeon with Lee Memorial Health System.
In a laparoscopic procedure surgeons operate through a series of poke holes, manually inserting thin cutting tools and a camera to provide magnified vision. It's used in a variety of surgical specialties.
"The vast majority of gallbladder surgeries are performed laparoscopically. A single incision in the belly button, one up under the breastbone and either one or two in the right upper side of the belly. Using long skinny instruments and looking up at a TV monitor, remove the gallbladder that way," says Dr. Miter.
While laparoscopic is a hands-on approach, robotic procedures are surgeon-controlled. Working at a console, surgeons direct the robotic arms, which have super-human capabilities and 3D, hi def vision.
"I mean you have to see it to believe it, that's a great tool to have. You got a very good depth perception. Plus the other thing when you're working with your hands it's more intuitive," says Dr. Nagesh Ravipati, colorectal surgeon with Lee Memorial Health System.
The robotic system performs maneuvers the human hand can't.
"Especially if you have to do any suturing, it is so much simpler with the robots because you can just turn around 360 degrees," says Dr. Ravipati.
Robotic surgery is gaining momentum in precise procedures, including the field of cancer.
"The robot is good when you're going to operate on just one field. For rectal surgery you're in one place, it's docked. It gives you the best 3 dimensional vision," says Dr. Ravipati.
Robotic and laparoscopic. Both cutting edge options, with less cutting.
View More Health Matters video segments at leememorial.org/healthmatters/
Lee Memorial Health System in Fort Myers, FL is the largest network of medical care facilities in Southwest Florida and is highly respected for its expertise, innovation and quality of care. For nearly a century, we've been providing our community with everything from primary care treatment to highly specialized care services and robotic assisted surgeries.
Visit leememorial.org
