- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
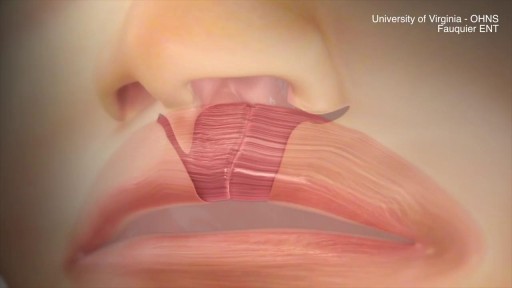
This animation demonstrates how a unilateral complete cleft lip repair is performed. This video is meant for educational purposes for patients and families. There are many ways to fix a complete cleft lip, but the technique shown here is the most common known as the Millard Rotation Advancement Repair.



Infected Hernia Mesh Repair Surgery Video
Ellis demonstrates how to insert and then remove an NG tube. This includes drawing gastric residual and checking the pH. After the demonstration, Ellis provides additional tips about clamping the NG tube and using the blue pigtail.
Our Critical Nursing Skills video tutorial series is taught by Ellis Parker MSN, RN-BC, CNE, CHS and intended to help RN and PN nursing students study for your nursing school exams, including the ATI, HESI and NCLEX.
#NCLEX #HESI #Kaplan #ATI #NursingSchool #NursingStudent #Nurse #RN #PN #Education #LVN #LPN #ClinicalSkills #NGTube #nurseeducator
00:00 What to expect
00:30 Preparing NG tube patient
00:56 Preparing NG tube equipment
1:29 Measuring the NG tube
2:02 Preparing for NG tube insertion
2:28 Inserting the NG tube
3:17 Checking placement with pH
4:23 Anchoring with split-tape
5:32 Connecting to suction
6:05 Disconnecting from suction
6:17 What to do before removal?
7:03 Removing NG tube
7:40 Additional tips on clamping
8:31 The blue pigtail
🚨 Reminder: shipping deadlines are looming 👀
🎁 Regular Shipping: Order by Friday, December 15
🚀 Expedited Shipping: Order by Monday, December 18
🔍 Still searching for last-minute gifts? Consider a Level Up RN Gift Card! 💌 It’s not only a thoughtful present but also the perfect way to share treasures like Pharmacology Flashcards OR digital treasures like Flashables Digital Nursing Flashcards & the Level Up RN membership. Give the gift of knowledge this holiday season! 🧠⚡️💖 bit.ly/LevelUpRNGC
🚪 Access our Cram Courses, Quizzes and Videos all in one ad free space with Level Up RN Membership https://bit.ly/LevelUpRNMembership
Want more ways to MASTER Clinical Skills? Check out our flashcards & videos!
👇👇👇👇👇👇👇👇👇👇
👉 https://bit.ly/clinicalnursingskills 👈
☝️👆☝️👆☝️👆☝️👆☝️👆
This is your one-stop-shop for materials to help you LEARN & REVIEW so you can PASS Nursing School.
🤔🤔🤔 DO YOU WANT TO PASS your classes, proctored exams and the NCLEX? 🤔🤔🤔 Our resources are the best you can buy. They are built with a single goal: help you pass with no fluff. Everything you need, and nothing you don’t. Don’t take our word for it, though! Check out our hundreds of ⭐️⭐️⭐️⭐️⭐️ reviews from nurses who passed their exams and the NCLEX with Level Up RN.
🗂️ Our Ultimate Nursing School Survival kit is your number 1 resource to get through nursing school and to pass the NCLEX. Whether you're just starting school or you’re already prepping for the NCLEX, this bundle of flashcards is the best you can buy. It covers all the information you need to know to pass all your exams and it has FREE shipping!
➡️ https://bit.ly/TUNSSK ⬅️
L👀king for EVEN MORE resources to survive Nursing School? Make your Nursing School experience your own! Life’s difficult enough—learning shouldn’t be.
🪅 Games https://nursesquad.com
💻 Digital resources https://bit.ly/NursingStudyCourses
📅 Organizational tools https://bit.ly/OrganizingSchool
✨Want perks? Join our channel!
https://youtube.com/leveluprn/join
🏷 Head to https://leveluprn.com/specials for all our latest deals!🥳️
📧 LOOKING FOR FREE RESOURCES TO HELP WITH YOUR EXAMS? Get exclusive tips, latest video releases and more delivered to your email!
➡️ https://leveluprn.com/signup ⬅️
⚕ 👩 LEVEL UP NURSE SQUAD 👩⚕️
All of the nurses at Level Up RN are here to help! Cathy Parkes started helping her fellow classmates back when she was in nursing school, tutoring so they could pass their exams and graduate. After she got her BSN and started working as an RN at Scripps Encinitas Hospital, she started this YouTube channel to help nursing students around the world. Since then she has built a team of top-notch dedicated nurses and nurse educators who are focused on improving nursing education and supporting career advancement for nurses everywhere. With flashcards, videos, courses, organizational tools and more, we are singularly focused on helping students and nurses Level Up on their exams and nursing careers.
✨This video is on the protein fibres of connective tissue, the types, structure and synthesis of collagen and elastin. I hope it helps! ☀️
🌟What's in this video?
0:00 - Intro
0:07 - Connective Tissue Recap
0:39 - Connective Tissue Fibres
1:22 - Collagen
1:46 - Types of Collagen
3:40 - Structure of Collagen
4:40 - Collagen Synthesis
8:50 - Elastin
✨ Other videos you may need:
🔅 Connective Tissue : https://youtu.be/xw_ALdt5n-A
🔅 Cartilage : https://youtu.be/4inWF4H6pKE
🔅Epithelial Tissue: https://youtu.be/Gw5fC0zXaeU
🔅Structure of Blood Vessels: https://youtu.be/BAo2UqqyL3g
🔅Histology: https://www.youtube.com/playli....st?list=PL1rG930trF2
💫 For more videos like this, subscribe to my channel!
Byte Size Med: https://youtube.com/channel/UC....ZghvlgylH3r_CWfA18eF
📚Factual References & for Further Reading:
- DiFiore's Atlas of Histology
- Junqueira's Basic Histology
- Harper's Biochemistry
- Gartner's Concise Histology
- Openstax Anatomy and Physiology
https://openstax.org/details/b....ooks/anatomy-and-phy
- Openstax Biology
https://openstax.org/details/books/biology-2e
(The last two are links to open-source references. They are NOT affiliate links)
🌤 Note:
These are just a collection of my notes. So use them the way you would use borrowed notes from a friend. 📝
The images in this video are hand-drawn for illustration and explanation only.✍️ Hence, they may not be anatomically accurate. I am just one person making these videos. If there are any errors, that is unintentional. I try super hard to avoid them. Please let me know if you find any, so it gets clarified for other viewers. Science constantly evolves and changes. New discoveries are made everyday. So some of the information in these videos may become outdated. If you notice that, please let me know so I can update them.
⚡️Disclaimer:
These videos are NOT a substitute for a medical textbook. Textbooks are written by experts (which I do not claim to be), edited, proofread and referenced. Please use them.
The information has been sourced from multiple references as mentioned above. I draw all the pictures myself. But if I have inadvertently infringed on any copyright, that is completely unintentional. I only make these videos to impart education. If I have accidentally violated copyright in any way, do let me know so I can make the necessary changes or give credit to anyone who is owed the same.
These videos are NOT intended for patient education. They are NOT a substitute for diagnosis and treatment by a licensed medical professional. Always seek the advice of a qualified health care provider for any questions you may have regarding any medical condition, so that they can address your individual needs.
🔅They are ONLY meant to help students of medicine and health sciences with studying, and should be used for just that purpose and absolutely nothing else.
Byte Size Med. All Rights Reserved.
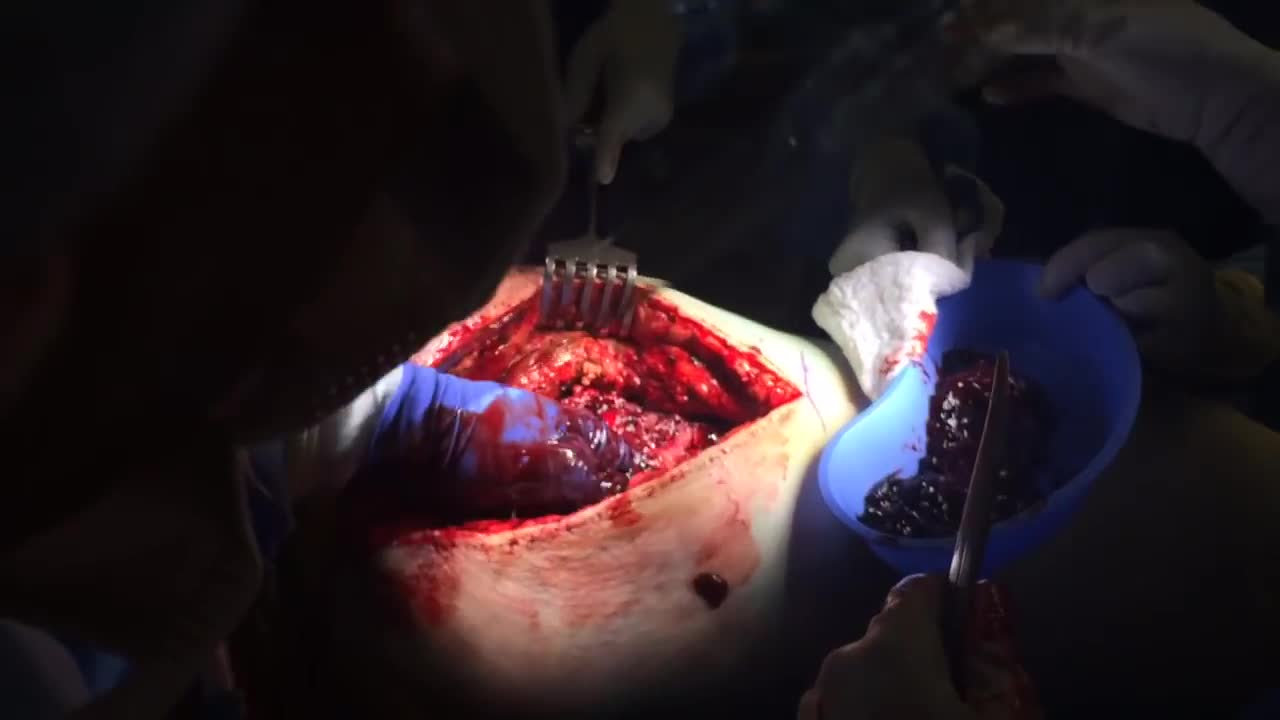
A hematoma is a common complication of surgical procedures. A large, expanding hematoma can result in necrosis of the overlying skin (1,2) or adjacent subcutaneous fat, increased incidence of infection, scarring, skin hyperpigmentation, tissue edema and a prolonged convalescence.

open multi puncture testicular biopsy to retrieve sperm for ICSI (IntaCytoplasmic Sperm Injection)

Most babies will move into delivery position a few weeks prior to birth, with the head moving closer to the birth canal. When this fails to happen, the baby’s buttocks and/or feet will be positioned to be delivered first. This is referred to as “breech presentation.” Breech births occur in approximately 1 out of 25 full-term births.

The most common symptoms of infection from animal bites are redness, pain, swelling, and inflammation at the site of the bite. You should seek immediate medical treatment if any of these symptoms continue for more than 24 hours. Other symptoms of infection include: pus or fluid oozing from the wound

Physical Examination of the abdomen

Loyola Full Male Exam Part 4 A video from Loyola medical school, Chicago showing the full examination of the male

Emergency C Section for a Bleeding Placenta

Watch that video to know What is Vaginal Discharge and How To Get Rid of It

Vaginoplasty is any surgical procedure that results in the construction or reconstruction of the vagina. It is a type of genitoplasty. Pelvic organ prolapse is often treated with one or more surgeries to repair the vagina.

UPMC liver surgeons are among the most experienced in the world in performing minimally invasive liver surgery. Most patients benefit from less trauma and pain, minimal scarring, a shorter hospital stay, and faster recovery than from traditional surgery.
To learn more, please visit https://www.upmc.com/services/....liver-cancer/treatme

How to Use Tampons for The First Time Demo Video

Ettore Vulcano, MD, Foot and Ankle Orthopedic Surgeon at Mount Sinai West, discusses a new minimally invasive bunion surgery that has patients walking immediately after surgery, and getting back to an active lifestyle much quicker than with the traditional surgery.

Please remember that this video is to be used for educational purposes. You must follow your facility or colleges' policies and procedure checklists to ensure you are completing the skill satisfactorily. Thanks for watching!
Music from #Uppbeat (free for Creators!):
https://uppbeat.io/t/swoop/blue-sea
License code: W9DFUQ4II7YVHA59

Injection in buttocks
