- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Uterine fibroids are the most common benign tumors and can affect one in three in Canada. While most fibroids are asymptomatic, they can cause heavy and painful periods, urinary frequency and urgency and pelvic discomfort and pain. A new treatment is available that doesn’t involve invasive surgery. With Fibristal, you can treat fibroids, relieve symptoms and finally live your life the way you want to!
Kawasaki disease is a condition that causes inflammation in the walls of medium-sized arteries throughout the body, including the coronary arteries, which supply blood to the heart muscle. Kawasaki disease is also called mucocutaneous lymph node syndrome because it also affects lymph nodes, skin, and the mucous membranes inside the mouth, nose and throat. Signs of Kawasaki disease, such as a high fever and peeling skin, can be frightening. The good news is that Kawasaki disease is usually treatable, and most children recover from Kawasaki disease without serious problems.

What is an Aneurysm? A cerebral or intracranial aneurysm is an abnormal focal dilation of an artery in the brain that results from a weakening of the inner muscular layer (the intima) of a blood vessel wall. The vessel develops a "blister-like" dilation that can become thin and rupture without warning. The resultant bleeding into the space around the brain is called a subarachnoid hemorrhage (SAH). This kind of hemorrhage can lead to a stroke, coma, and/or death. Aneurysms are usually found at the base of the brain just inside the skull, in an area called the subarachnoid space. In fact, 90 percent of SAHs are attributed to ruptured cerebral aneurysms and the two terms are often used synonymously.
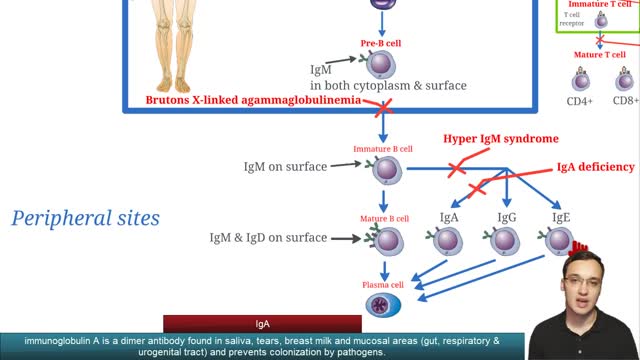
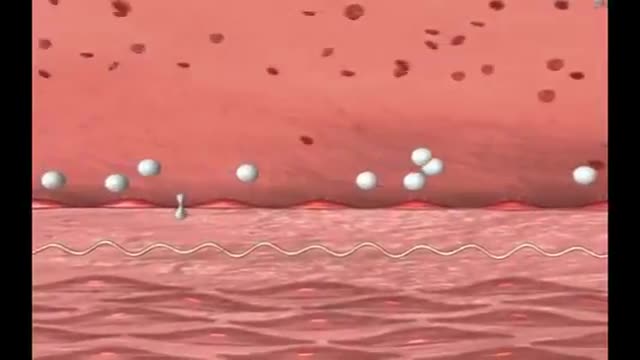
Selective immunoglobulin A deficiency (SIgAD) is a primary immunodeficiency disease and is the most common of the primary antibody deficiencies.[1] Total immunoglobulin A deficiency (IgAD) is defined as an undetectable serum immunoglobulin A (IgA) level at a value < 5 mg/dL (0.05 g/L) in humans. Partial IgAD refers to detectable but decreased IgA levels that are more than 2 standard deviations below normal age-adjusted means.[2, 3] IgAD is commonly associated with normal B lymphocytes in peripheral blood, normal CD4+ and CD8+ T cells, and, usually, normal neutrophil and lymphocyte counts. Anti-IgA autoantibodies of the IgG and/or IgE isotype may be present. Peripheral blood may also be affected by autoimmune cytopenias, eg, autoimmune thrombocytopenia,[4, 5] and patients may have other autoimmune phenomena. IgA was first identified by Graber and Williams in 1952; ten years later, the first patients with IgAD were described. IgAD is a heterogeneous disorder, and the results of intensive study are beginning to elucidate genetic loci and molecular pathogenesis that contribute to various subtypes of this disorder. Several lines of evidence suggest that, in many cases, IgAD and common variable immunodeficiency (CVID) have a common pathogenesis, which is discussed further in Pathophysiology. Other data indicate different genetic risk factors. Family studies show variable inheritance patterns. Familial inheritance of IgAD occurs in approximately 20% of cases,[6] and, within families, IgAD and CVID are associated.[7, 8] Many IgAD patients are asymptomatic (ie, "normal" blood donors) and are identified by finding a laboratory abnormality, without any apparent associated clinical disease. Some patients with IgAD may have the following associated conditions: (1) deficits in one or more immunoglobulin G (IgG) subclasses (this accounts for 20-30% of IgA-deficient patients, many of whom may have total IgG levels within the normal range) or (2) a deficient antibody response to pneumococcal immunization (specific polysaccharide antibody deficiency [SPAD]). Some patients with IgAD later develop CVID, and family members of patients with CVID may have only selective IgAD. Characterization of the receptor for the transmembrane activator and calcium-modulator and cyclophilin ligand interactor (TACI), encoded by the gene TNFRSF13B ( tumor necrosis factor receptor superfamily member 13B), suggests that people with the C104, A181E, and ins204A variants may be at risk for IgAD that progresses to CVID.[9] Primary IgAD is permanent, and below-normal levels have been noted to remain static and persist after 20 years of observation.[10] A recent report documents a rare case of reversion.[11] Environmental factors such as drugs or infections can cause IgAD, but this form is reversible in more than half the cases (see Causes). Although individuals with IgAD have largely been considered healthy, recent studies indicate a higher rate of symptoms. A 20-year follow-up study that compared 204 healthy blood donors with incidentally identified IgAD to 237 healthy subjects with normal IgA levels demonstrated that 80% of IgAD donors and 50% of control subjects had episodes of infections, drug allergy, or autoimmune or atopic disease. Severe respiratory tract infections occurred in 26% of IgAD subjects, in 24% of subjects with decreased IgA levels, and in 8% of control subjects; however, the incidence of life-threatening infections was not increased. IgAD is more common in adult patients with chronic lung disease than in healthy age-matched control subjects.[12] Patients with IgAD are at some increased risk of developing severe reactions after receiving blood products.[13, 14, 15] IgG anti-IgA antibodies may cause severe transfusion reactions if patients with IgAD are given whole blood; therefore, IgA-poor blood or washed red cells are preferred for those patients. IgA-deficient patients with immunoglobulin E (IgE)–class anti-IgA antibodies are at risk for anaphylaxis if they receive blood or intravenous immunoglobulin, but this situation is extremely rare. Individuals with such an unusual profile should receive only low IgA intravenous immunoglobulin preparations. However, caution must be used when administering IGIV to patients with IgAD if their anti-IgA status is unknown. A history devoid of previous blood product administration does not exclude the possibility of anti-IgA antibodies or adverse reactions. Fortunately, appropriate precautions can significantly reduce morbidity (see Treatment). Blood banks can use a simple ELISA screening approach to establish an IgAD blood donor poo
Fainting occurs when the blood supply to your brain is momentarily inadequate, causing you to lose consciousness. This loss of consciousness is usually brief. Fainting can have no medical significance, or the cause can be a serious disorder. Therefore, treat loss of consciousness as a medical emergency until the signs and symptoms are relieved and the cause is known. Discuss recurrent fainting spells with your doctor. If you feel faint Lie down or sit down. To reduce the chance of fainting again, don't get up too quickly. Place your head between your knees if you sit down. If someone else faints Position the person on his or her back. If the person is breathing, restore blood flow to the brain by raising the person's legs above heart level — about 12 inches (30 centimeters) — if possible. Loosen belts, collars or other constrictive clothing. To reduce the chance of fainting again, don't get the person up too quickly. If the person doesn't regain consciousness within one minute, call 911 or your local emergency number. Check the person's airway to be sure it's clear. Watch for vomiting. Check for signs of circulation (breathing, coughing or movement). If absent, begin CPR. Call 911 or your local emergency number. Continue CPR until help arrives or the person responds and begins to breathe.
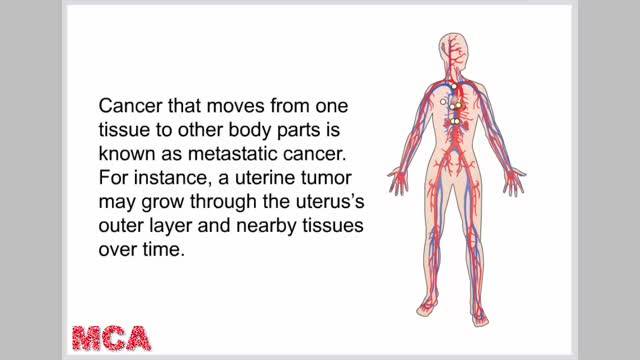
The uterus, or womb, is an important female reproductive organ. It is the place where a baby grows when a women is pregnant. There are different types of uterine cancer. The most common type starts in the endometrium, the lining of the uterus. This type of cancer is sometimes called endometrial cancer. The symptoms of uterine cancer include Unusual vaginal bleeding or discharge Trouble urinating Pelvic pain Pain during intercourse Uterine cancer usually occurs after menopause. Being obese and taking estrogen-alone hormone replacement therapy (also called menopausal hormone therapy) also increase your risk. Treatment varies depending on your overall health, how advanced the cancer is and whether hormones affect its growth. Treatment is usually a hysterectomy, which is surgery to remove the uterus. The ovaries and fallopian tubes are also removed. Other options include hormone therapy and radiation.
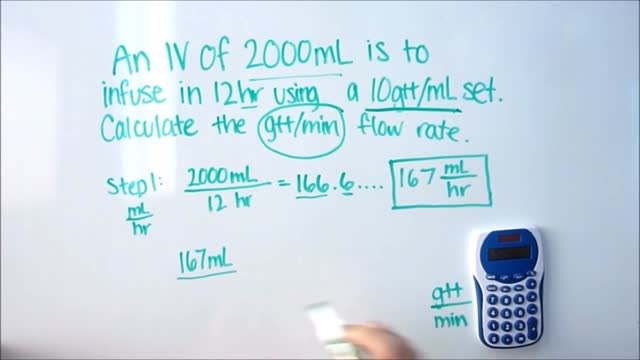
IV Dose Calculations

Cardiac arrest is the abrupt loss of heart function in a person who may or may not have diagnosed heart disease. The time and mode of death are unexpected. It occurs instantly or shortly after symptoms appear. Each year, more than 350,000 emergency medical services-assessed out-of-hospital cardiac arrests occur in the United States

Sclerotherapy is a procedure used to eliminate varicose veins and spider veins. Sclerotherapy involves an injection of a solution (generally a salt solution) directly into the vein. The solution irritates the lining of the blood vessel, causing it to collapse and stick together and the blood to clot.Sep 17, 2016
Exercises. Light exercises in which you move your affected limb may encourage lymph fluid drainage and help prepare you for everyday tasks, such as carrying groceries. ...

The temporomandibular joint (TMJ), located just in front of the lower part of the ear, allows the lower jaw to move. The TMJ is a ball-and-socket joint, just like the hip or shoulder. When the mouth opens wide, the ball (called the condyle) comes out of the socket and moves forward, going back into place when the mouth closes. TMJ becomes dislocated when the condyle moves too far and gets stuck in front of a bony prominence called the articular eminence. The condyle can't move back into place. This happens most often when the ligaments that normally keep the condyle in place are somewhat loose, allowing the condyle to move beyond the articular eminence. The surrounding muscles often go into spasm and hold the condyle in the dislocated position.

DIRTIEST PARTS OF YOUR BODY
Hearing loss can affect anyone at any age, due to heredity, medical conditions or loud noise exposure. However, as we get older, we naturally become more susceptible to hearing loss because of changes to the delicate mechanics of our ears.

The ACL is one of the four main ligaments within the knee that connect the femur to the tibia. The knee is essentially a hinged joint that is held together by the medial collateral (MCL), lateral collateral (LCL), anterior cruciate (ACL) and posterior cruciate (PCL) ligaments.
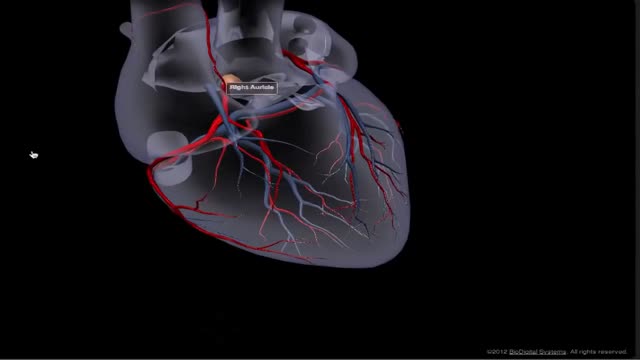
The heart receives its own supply of blood from the coronary arteries. Two major coronary arteries branch off from the aorta near the point where the aorta and the left ventricle meet. These arteries and their branches supply all parts of the heart muscle with blood.
What could cause a blockage in the stomach? Mechanical causes of intestinal obstruction may include: Adhesions or scar tissue that forms after surgery. Foreign bodies (objects that are swallowed and block the intestines) Gallstones (rare) Hernias. Impacted stool. Intussusception (telescoping of one segment of bowel into another) Tumors blocking the intestines. Less common radiologic signs are seen in specific circumstances. Most closed-loop obstructions (75%) are caused by adhesions. A closed-loop obstruction occurs when a loop of bowel is not decompressed by the caudal passage of gas and fluid.

Myasthenia gravis is a chronic autoimmune neuromuscular disease characterized by varying degrees of weakness of the skeletal (voluntary) muscles of the body. The name myasthenia gravis, which is Latin and Greek in origin, literally means "grave muscle weakness."

Controlled studies on treatment of catscratch disease (CSD) are lacking. Thus, treatment recommendations are based on case reports, reviews, a single controlled trial, and anecdotal data. Practice guidelines for the diagnosis and management of skin and soft-tissue infections, including CSD, have been established.Oct 19, 2016
A hormone is a chemical messenger that enables communication between cells. Hormones are secreted by the glands of the endocrine system and they serve to maintain homeostasis and to regulate numerous other systems and processes, including reproduction and development.

irregular, curved toenails. footwear that places a lot of pressure on the big toes, such as socks and stockings that are too tight or shoes that are too tight, narrow, or flat for your feet. toenail injury, including stubbing your toe, dropping something heavy on your foot, or kicking a ball repeatedly. poor posture. How can ingrowing toenails be prevented? Cut your nails straight across; do not cut them too short or too low at the sides. ... Keep your feet clean and dry. ... Avoid tight shoes and use cotton socks rather than synthetic. If you have diabetes, you should take extra care when cutting your nails:
