- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
This medication is used to treat certain types of serious (possibly fatal) irregular heartbeat (such as persistent ventricular fibrillation/tachycardia). It is used to restore normal heart rhythm and maintain a regular, steady heartbeat. Amiodarone is known as an anti-arrhythmic drug. It works by blocking certain electrical signals in the heart that can cause an irregular heartbeat.
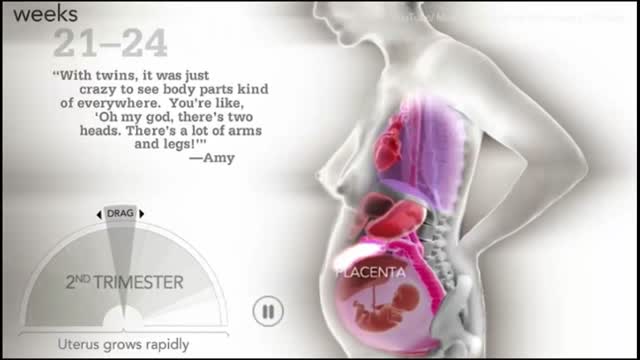
How a woman's body changes during Pregnancy

One technique to relocate a dislocated elbow with anatomy diagrammed out.

Cardiac arrest is the abrupt loss of heart function in a person who may or may not have diagnosed heart disease. The time and mode of death are unexpected. It occurs instantly or shortly after symptoms appear. Each year, more than 350,000 emergency medical services-assessed out-of-hospital cardiac arrests occur in the United States

Factitious disorder is the term used to describe a pattern of behavior centered on the exaggeration or outright falsifications of one’s own health problems or the health problems of others. Some people with this disorder fake or exaggerate physical problems; others fake or exaggerate psychological problems or a combination of physical and psychological problems. Factitious disorder differs from a pattern of falsified or exaggerated behavior called malingering. While malingerers make their claims out of a motivation for personal gain, people with factitious disorder have no such motivation.

Furosemide is a prescription drug. It’s available in two forms that you take by mouth: a tablet and a solution. It’s also available as an injectable solution, which is given by a healthcare provider. The furosemide tablet is available as the brand-name drug Lasix. It’s also available as a generic drug. Generic drugs usually cost less. In some cases, they may not be available in every strength or form as the brand-name version.


During this week your baby's brain form channels and creases with the help of more tissues with greater surface area. Check out this video for detail information on 30 weeks pregnant -

Liver transplantation is surgery to remove a diseased or injured liver and replace it with a healthy whole liver or a segment of a liver from another person, called a donor. People with either acute or chronic liver failure may need a liver transplant to survive.

DIRTIEST PARTS OF YOUR BODY
Interventional Nephrology is a new and emerging subspecialty of Nephrology that mainly deals with ultrasonography of kidneys and ultrasound-guided renal biopsy, insertion of peritoneal dialysis catheters, tunneled dialysis catheters as a vascular access for patients undergoing hemodialysis as well as percutaneous ...
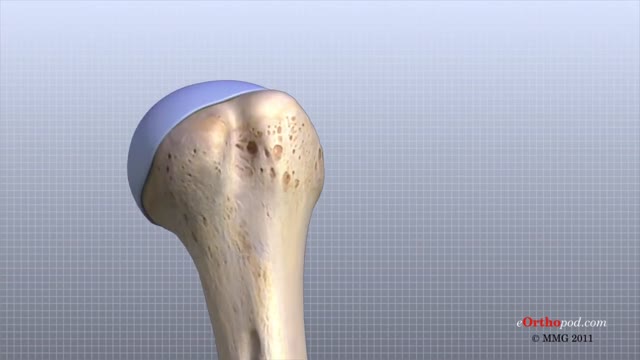
The shoulder joint is formed where the humerus (upper arm bone) fits into the scapula (shoulder blade), like a ball and socket. Other important bones in the shoulder include: The acromion is a bony projection off the scapula. The clavicle (collarbone) meets the acromion in the acromioclavicular joint.

Hold your elbows at shoulder level and place the backs of your hands together with your wrists bent at 90 degrees. This position increases the pressure on the median nerve. If the test reproduces or worsens your symptoms (pain and tingling in your hands), you may have carpal tunnel syndrome.
Pancreatic Auto Islet Transplantation is a procedure used to maintain insulin production and secretion in patients with chronic pancreatitis that are undergoing a total pancreatectomy, or removal of the entire pancreas. When all other medical therapies fail to control the pain, removal of the pancreas may be an option; however it can leave a person diabetic, which means that the body can no longer control blood sugar levels, and will require intensive testing of blood sugar and injections of insulin. The pancreas is an organ, located in the upper abdominal cavity, behind the stomach, liver and colon. Within the pancreas, specialized clusters of cells known as islets produce insulin, which maintain healthy blood sugar levels. The pancreas also produces enzymes to help digest food. In order to alleviate pain and maintain insulin production, the pancreas is removed from the body, processed and the islets are harvested. Once the pancreas is removed, it is placed in a solution and put into a machine where the pancreas is digested. The islets are then infused into the patient’s liver. Within a short time, the islets are expected to start producing insulin. In 80% of patients, the pain from pancreatitis is relieved by a total pancreatectomy. Over time, some patients may be diabetic and will need to take insulin to maintain healthy blood sugar levels. All patients will take pancreatic enzymes to help digest food after surgery.
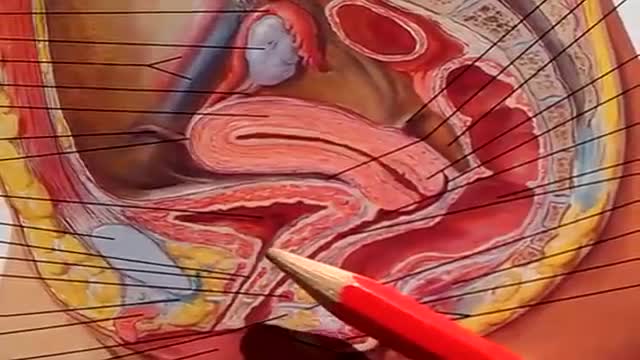
The urinary bladder is a hollow muscular organ that collects urine from the kidneys before disposal by urination. A hollow muscular, and distensible (or elastic) organ, the bladder sits on the pelvic floor. Urine enters the bladder via the ureters and exits via the urethra.

Your egg usually lives for just 12 to 24 hours, but sperm will live inside you for anything from a few hours to seven days, with one to three days the optimum time. ... But because a small number of sperm are long-living, having sex up to six days before ovulation can also result in pregnancy.
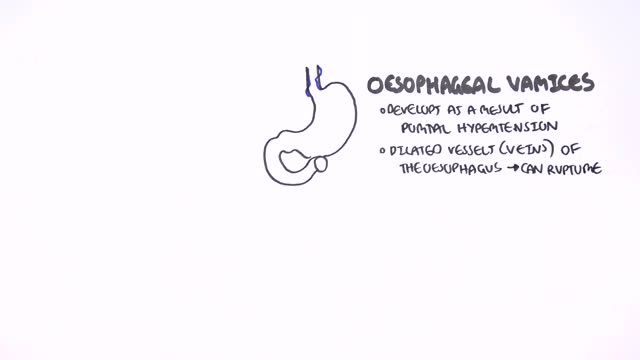
This could be caused by an infection, food poisoning, parasites, Crohn's disease, or reduced blood flow in the colon. Hemorrhoids are another common cause of GI or rectal bleeding. A hemorrhoid is an enlarged vein in your rectum or anus. These enlarged veins can rupture and bleed, causing rectal bleeding.

Watch that video to know if it is safe to have sex during period or not
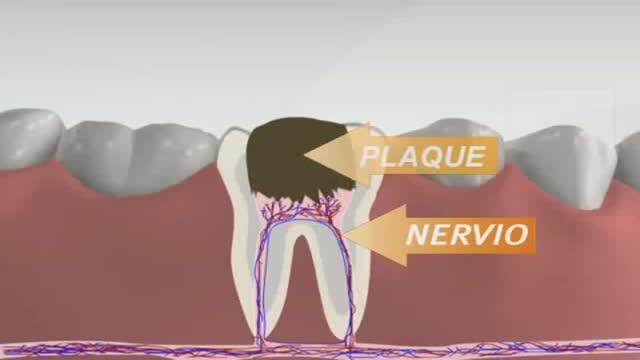
Root canals are common procedures and can help save your tooth from extraction. Dentists at Aspen Dental practices have been safely and expertly performing root canal procedures for over two decades.
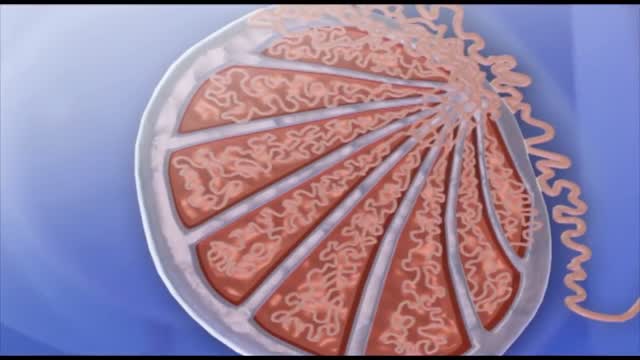
Spermatogenesis is the process in which spermatozoa are produced from spermatogonial stem cells by way of mitosis and meiosis. The initial cells in this pathway are called spermatogonia, which yield primary spermatocytes by mitosis.
