- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Spina bifida is a condition that affects the spine and is usually apparent at birth. It is a type of neural tube defect (NTD). Spina bifida can happen anywhere along the spine if the neural tube does not close all the way. When the neural tube doesn’t close all the way, the backbone that protects the spinal cord doesn’t form and close as it should. This often results in damage to the spinal cord and nerves. Spina bifida might cause physical and intellectual disabilities that range from mild to severe. The severity depends on: The size and location of the opening in the spine. Whether part of the spinal cord and nerves are affected.

During open-heart valve surgery, the doctor makes a large incision in the chest. Blood is circulated outside of the body through a machine to add oxygen to it (cardiopulmonary bypass or heart-lung machine). The heart may be cooled to slow or stop the heartbeat so that the heart is protected from damage while surgery is done to replace the valve with an artificial valve. The artificial valve might be mechanical (made of man-made substances). Others are made out of animal tissue, often from a pig.

Posterior dislocations with associated fractures, also known as complex posterior dislocations, often require open reduction and fixation (ORIF). These dislocations are often associated with significant ligamentous injury. In some cases, complex posterior elbow dislocations may be managed with closed reduction. Posterior elbow dislocations that are neglected, as is not uncommon in developing countries, can often be effectively treated with open reduction. [9] Delayed vascular compromise is an important complication after reduction. All patients should be observed for a period of approximately 2-3 hours after reduction. If no evidence of vascular compromise arises, patients can be sent home with appropriate follow-up and instructions to watch for further problems.

- elbow dislocations in children are a relatively uncommon; - peak incidence occurs in adolescence between 11-15 years. - posterior dislocations are most common type; - posterior dislocation usually results from fall on outstretched hand w/ forarm supinated & elbow extended or partially flexed; - coronoid process, which nl resists posterior displacement of ulna, is relatively small in children; - anterior capsule of elbow joint is torn by force of the impact transmitted upward thru the ulna and radius
Watch that video of Unbelievable Mutations and Medical Condition Photos

Anxiety Disorder, How To Calm Anxiety, Beck Anxiety Inventory, Best Anxiety Medication ---- http://panic-attacks-anxiety.good-info.co --- They’re calling it the “Anxiety Destroyer Technique” Check it out... Last week I told you I stumbled upon a video presentation that teaches a simple trick to stop your next panic attack... and relieve high anxiety levels… in 60 seconds or less... Well, it seems the folks who have tried this technique already are amazed by it. In fact, some are so blown away by how much relief they’re enjoying that they’re now calling this little trick... the “Anxiety Destroyer Technique”. So guess what? I did some research. Turns out its not some Hocus-Pocus solution. It’s actually based on a revolutionary new clinically proven form of therapy, called Neuro Activation Therapy! This technique is unlike anything I’ve seen or heard about before. It has nothing to do with drugs breathing exercises, or anything you’ll read about in a book or website online. Best part: It’s not just a solution for panic attacks and anxiety. The same technique works on fears phobias, overwhelming levels or stress and worry, obsessive-compulsive disorder, social anxiety – even depression! I highly recommend you this technique. If you suffer from these issues, it really can help you. Click Here: http://panic-attacks-anxiety.good-info.co
Methotrexate anti-tumor activity is a result of the inhibition of folic acid reductase, leading to inhibition of DNA synthesis and inhibition of cellular replication. The mechanism involved in its activity against rheumatoid arthritis is not known.
Breast Implants Bottoming Out? Steps to Reduce The Risks
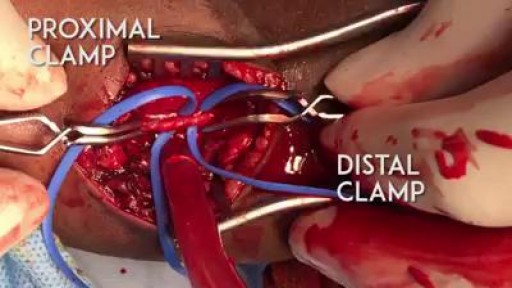
A proper embolectomy should have a good proximal and distal flow to the arteriotomy :)
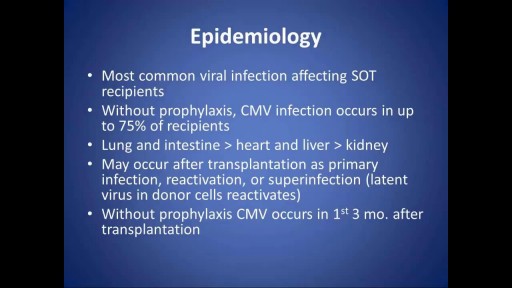
Cytomegalovirus (CMV) continues to have a tremendous impact in solid organ transplantation despite remarkable advances in its diagnosis, prevention and treatment. It can affect allograft function and increase patient morbidity and mortality through a number of direct and indirect effects. Patients may develop asymptomatic viremia, CMV syndrome or tissue-invasive disease. Late-onset CMV disease continues to be a major problem in high-risk patients after completion of antiviral prophylaxis. Emerging data suggests that immunologic monitoring may be useful in predicting the risk of late onset CMV disease. There is now increasing interest in the development of an effective vaccine for prevention. Novel antiviral drugs with unique mechanisms of action and lesser toxicity are being developed. Viral load quantification is now undergoing standardization, and this will permit the generation of clinically relevant viral thresholds for the management of patients. This article provides a brief overview of the contemporary epidemiology, clinical presentation, diagnosis, prevention and treatment of CMV infection in solid organ transplant recipients.


Face Lift Surgery Proceure

Teeth whitening fit for a beauty queen! Miss. Harris County Teen Angela H. just completed a ZOOM! whitening.

Veryyyyy funny!

Things nurses should know about their patients. As a new nurse, it can be hard trying to determine what information you need to know during your shift. In addition, nurses can get extremely busy and strapped for time, so how do you keep up with all of the things you need to know?
🟣Nursing Resume Templates and Job Guide🟣
eBook: https://registerednursern.creator-spring.com/
Paperback: https://amzn.to/3QvzH3W (affiliate ad)
Free Report Sheet Templates: https://www.registerednursern.....com/nursing-report-s
In this video, Nurse Sarah explains some of the most important things nurses need to know about their patients. However, these things can vary depending on your specialty and patient population. These tips are designed to help new nurses begin to think like a nurse.
Some examples of thing nurses should know about their patients include their allergies, code status, diagnosis, medications, vital signs, and much more.
Website: https://www.registerednursern.com/
More Videos: https://www.youtube.com/watch?v=R2XMro13dD0&list=UUPyMN8DzkFl2__xnTEiGZ1w
Nursing Gear: https://teespring.com/stores/registerednursern
Instagram: https://www.instagram.com/registerednursern_com/
Facebook: https://www.facebook.com/RegisteredNurseRNs
Twitter: https://twitter.com/NursesRN
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Hysterectomy done laparoscopically is a relative new approach to the classical hysterectomy procedure, the advantages are better anatomic views, less bleeding, less surgical time and less recovery time

Sensory and reflexes exam of the upper limb from the USMLE collection Sensory and reflexes exam of the upper limb
