- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Hysterectomy done laparoscopically is a relative new approach to the classical hysterectomy procedure, the advantages are better anatomic views, less bleeding, less surgical time and less recovery time

Sensory and reflexes exam of the upper limb from the USMLE collection Sensory and reflexes exam of the upper limb

Cerebellar functions of the lower limbs from the USMLE collection

Part 2: from Loyola Medical School, Chicago showing clinical examination of the neurological system.
Ultra Sound-Guided Interscalene Block
Modern technique of thyroidectomy for tumors

Teeth digital X-Ray

19 years old young man with inguinoscrotal right hernia.Decision-making for repair with minimal prosthetic residual material, and no stitches use for best comfort

Atrial Fibrillation is the most common heart rythmn abnormatlity and is very common as you age. Atrial fibrillation is a condition in which the top chambers of the heart, the Atrium are fibrillating, rather than having a regular synchronized contraction. One of the worst complications of Atrial Fibrillation can be Stroke. There are very good treatments of Atrial Fibrillation. This animated video is an overview of Atrial Fibrillation.
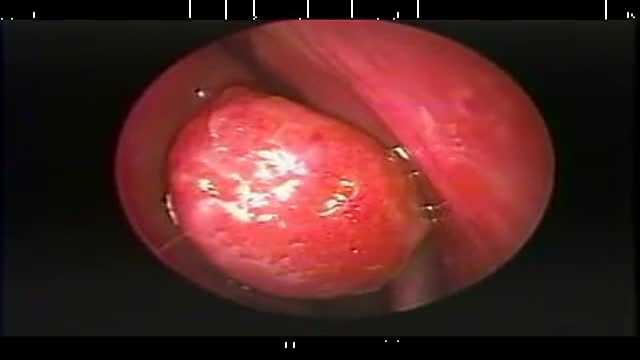
Endoscopic resection of a large right concha bullosa.

Homan's sign for deep vein thrombosis

Cosmetic surgery-mammoplasty-breast surgery-tummy

Video shows a Hip resurfacing operation done using the Durom hip from Zimmer.
The patient is a young active male. Hip resurfacing is emerging as the surgical procedure of choice in young and active patients for pain relief from Hip arthritis.

The video will describe mediastinal structures as they are seen on X-ray. Please see web site for disclaimer.

esophago-gastro- duodinoscopy
Gastroduodinoscopy requires special training and considerable experience but affords valuable information.
By its implement the whole of the interior of the stomach as well as esophagus, the first part and the proximal section of the second part of the duodenum and both efferent and afferent loops of the gastrojujenostomy if present can be scrutinized.
Gastroscopy is valuable in the diagnosis of gastric ulcers, in checking the results of medical treatment of chronic gastric ulcer. Gastroduodinoscopy is valuable in differential diagnosis between chronic peptic ulcer and gastric carcinoma, in diagnosis of small gastric neoplasm, in the detection of certain forms of gastritis, in examination of a stoma, in cases of gastrojujenostomy, in cases of duodinitis and duodenal ulcer.
Now its' the Era of
VIDEOGASROSCOPE
Direct means of diagnosis of upper G.I. diseases
Continuous Video recording of the entire procedure is there by which
we can review the whole procedure by playing the Video.
We are doing final diagnosis of upper G.I. lesions with biopsy.
Treatment becomes easy and to the point.
Early detection of pre malignant and malignant lesions is appreciable.

DMC Pediatric Orthopaedic Surgery specialist repairs a youg girl's traumatic spine injury. ~ Detroit Medical Center

Arterial line insertion usually involves cannulation of the radial artery with a 20 gauge catheter for the purposes of beat-by-beat blood pressure monitoring all along with arterial blood gas monitoring.
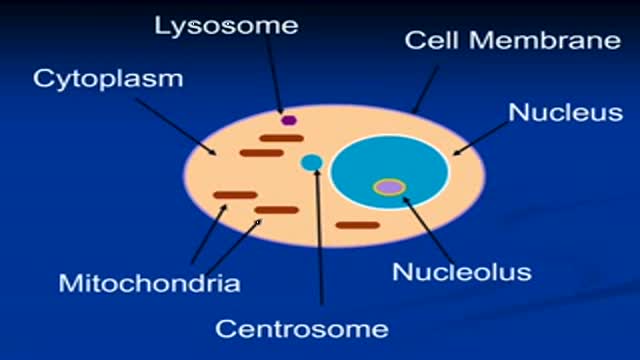
The video will describe aerobic and anaerobic metabolim in mitochondria. Please visit my website for disclaimer.

peptic ulcer

Headaches with eating Ice Cream explained by medicine
