- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
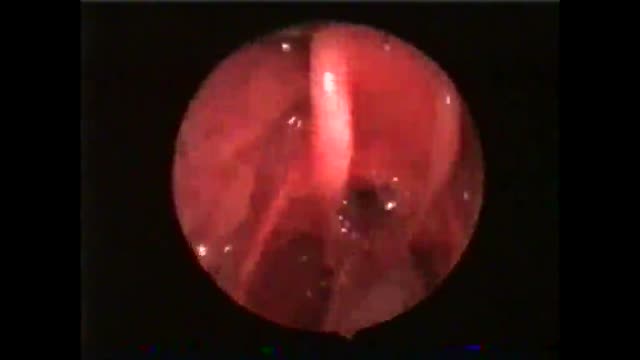
This patient swallows with the endotracheal tube in situ.He is not yet in the late stage of anaesthesia. Unfortunately, this may lead to intubation granuloma later on.

A high definition medical video showing the Laparoscopic inguinal hernia repair

Anatomy of The Ear

Anatomy of The Peritoneal Cavity

Diabetic Nephropathy Animation 3D

Pterygium Excision with Auto Conjunctival Graft

Robyn Benincasa, an extreme sports adventure racer, marathoner and firefighter maintains her active lifestyle following a hip replacement at St. Vincent Medical Center's Joint Replacement Institute with Dr. Thomas Schmalzried in Los Angeles, California. For more information, please visit: www.jri-docs.com

The term mallet finger has long been used to describe the deformity produced by disruption of the terminal extensor mechanism at the distal interphalangeal (DIP) joint. Mallet finger is the most common closed tendon injury that is seen in athletes; this injury is also common in nonathletes after "innocent" trauma. Mallet finger has also been referred to as drop, hammer, or baseball finger (although baseball accounts for only a small percentage of such injuries).
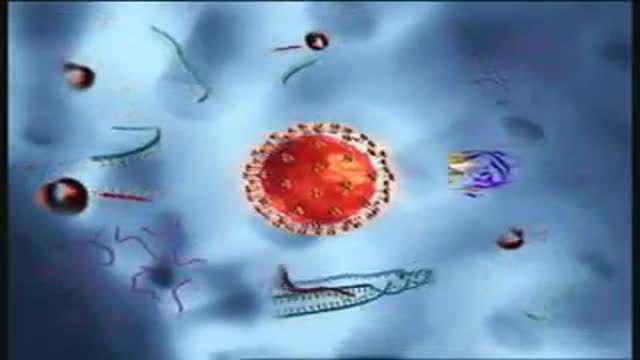
Binding and Fusion: HIV begins its life cycle
when it binds to a CD4 receptor and one of two
co-receptors on the surface of a CD4+
Tlymphocyte. The virus then fuses with the host
cell. After fusion, the virus releases RNA, its
genetic material, into the host cell.
Reverse Transcription: An HIV enzyme
called reverse transcriptase converts the singlestranded HIV RNA to double-stranded HIV DNA.
Integration: The newly formed HIV DNA
enters the host cell's nucleus, where an HIV
enzyme called integrase "hides" the HIV DNA
within the host cell's own DNA. The integrated
HIV DNA is called provirus. The provirus may
remain inactive for several years, producing few or
no new copies of HIV
Transcription: When the host cell receives a
signal to become active, the provirus uses a host
enzyme called RNA polymerase to create copies of
the HIV genomic material, as well as shorter
strands of RNA called messenger RNA (mRNA).
The mRNA is used as a blueprint to make long
chains of HIV proteins.
Assembly: An HIV enzyme called protease cuts
the long chains of HIV proteins into smaller
individual proteins. As the smaller HIV proteins
come together with copies of HIV's RNA genetic
material, a new virus particle is assembled.
Budding: The newly assembled virus pushes out
("buds") from the host cell. During budding, the new
virus steals part of the cell's outer envelope. This
envelope, which acts as a covering, is studded with
protein/sugar combinations called HIV
glycoproteins. These HIV glycoproteins are
necessary for the virus to bind CD4 and coreceptors. The new copies of HIV can now move
on to infect other cells.
What Causes Chest Pain ?
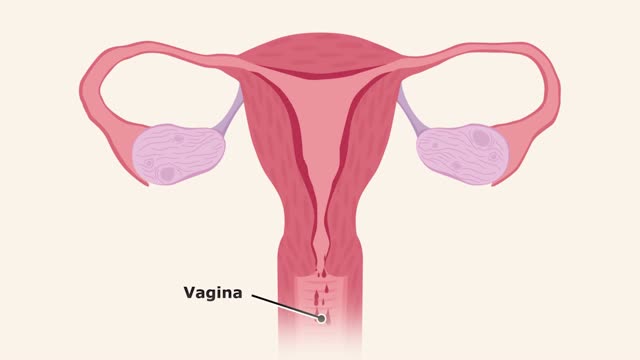
The menstrual cycle is the monthly series of changes a woman's body goes through in preparation for the possibility of pregnancy. Each month, one of the ovaries releases an egg — a process called ovulation. At the same time, hormonal changes prepare the uterus for pregnancy.
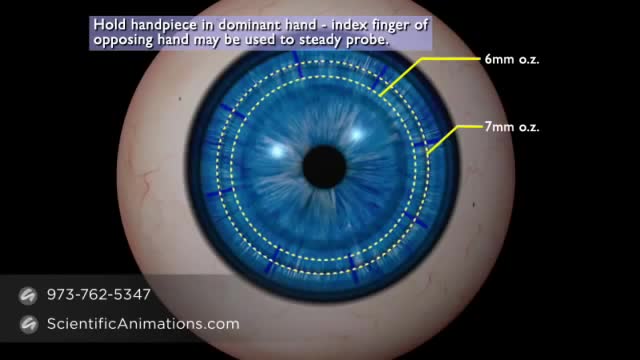
A cornea transplant, also called keratoplasty, is a surgical procedure to replace part of your cornea with corneal tissue from a donor. Your cornea is the transparent, dome-shaped surface of your eye that accounts for a large part of your eye's focusing power. A cornea transplant can restore vision, reduce pain and improve the appearance of a damaged or diseased cornea. Most cornea transplant procedures are successful. But cornea transplant carries a small risk of complications, such as rejection of the donor cornea.
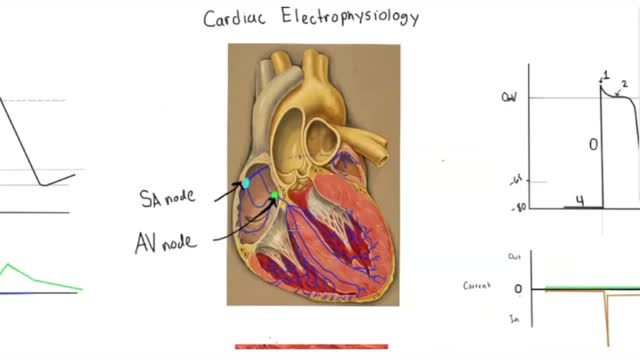
Electrophysiology studies test the electrical activity of your heart to find where an arrhythmia (abnormal heartbeat) is coming from. These results can help you and your doctor decide whether you need medicine, a pacemaker, an implantable cardioverter defibrillator (ICD), cardiac ablation or surgery.

OverviewSymptomsTestingComplicationsTreatmentPreventionTakeawayRead This Next What is gonorrhea? Highlights Some people may never develop noticeable symptoms. Gonorrhea is usually treated with an antibiotic injection or oral antibiotics. You’re at a higher risk of contracting gonorrhea if you’ve had any other STDs. Gonorrhea is a sexually transmitted disease (STD). It’s caused by infection with the bacterium Neisseria gonorrhoeae. It tends to infect warm, moist areas of the body, including the: urethra (the tube that drains urine from the urinary bladder) eyes throat vagina anus female reproductive tract (the fallopian tubes, cervix, and uterus) Gonorrhea passes from person to person through unprotected oral, anal, or vaginal sex. People with numerous sexual partners or those who don’t use a condom are at greatest risk of infection. The best protections against infection are abstinence, monogamy (sex with only one partner), and proper condom usage. Behaviors that make a person more likely to engage in unprotected sex also increase the likelihood of infection. These behaviors include alcohol abuse and illegal drug abuse, particularly intravenous drug use. Advertisement Symptoms of gonorrhea Symptoms
Depression (major depressive disorder or clinical depression) is a common but serious mood disorder. It causes severe symptoms that affect how you feel, think, and handle daily activities, such as sleeping, eating, or working. To be diagnosed with depression, the symptoms must be present for at least two weeks.

Slicosis is caused by inhalation of unbound (free) crystalline silica dust and is characterized by nodular pulmonary fibrosis. Chronic silicosis initially causes no symptoms or only mild dyspnea but over years can advance to involve most of the lung and cause dyspnea, hypoxemia, pulmonary hypertension, and respiratory impairment. Diagnosis is based on history and chest x-ray findings. No effective treatment exists except supportive care and, for severe cases, lung transplantation.
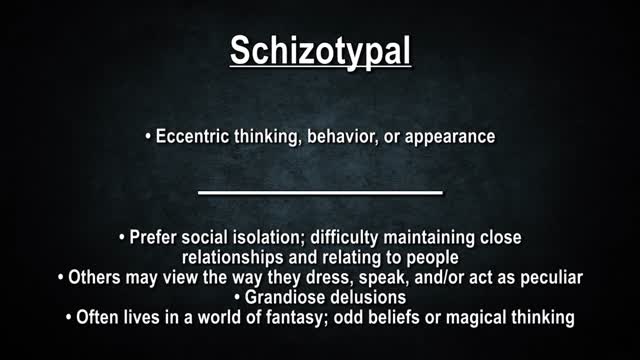
Personality disorders are a group of mental illnesses. They involve long-term patterns of thoughts and behaviors that are unhealthy and inflexible. The behaviors cause serious problems with relationships and work. People with personality disorders have trouble dealing with everyday stresses and problems. They often have stormy relationships with other people. The cause of personality disorders is unknown. However, genes and childhood experiences may play a role. The symptoms of each personality disorder are different. They can mild or severe. People with personality disorders may have trouble realizing that they have a problem. To them, their thoughts are normal, and they often blame others for their problems. They may try to get help because of their problems with relationships and work. Treatment usually includes talk therapy and sometimes medicine.

A heart attack occurs when the flow of blood to the heart is blocked, most often by a build-up of fat, cholesterol and other substances, which form a plaque in the arteries that feed the heart (coronary arteries). The interrupted blood flow can damage or destroy part of the heart muscle. A heart attack, also called a myocardial infarction, can be fatal, but treatment has improved dramatically over the years. It's crucial to call 911 or emergency medical help if you think you might be having a heart attack
One of the most common parasites to infect human beings is the yeast-like Blastocystis hominis, a single-celled parasitic organism that causes abdominal cramping, bloating, gas, and sometimes anal itching. Other common parasites are: Tapeworms, which can grow as long as 60 feet while living in the human intestines.

Inner Workings tells the story of the ceaseless pull of the human heart — even as it works against the very stoic realism of the brain.
