- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Some of these advancements include the use of robots to perform the surgery and the use of computer mapping scanners and software and even 3D printers to make the artificial knee implant. We are also seeing a lot of different advances being made by the medical device manufacturers.Some of these changes are designed to make the devices more durable than the 10 to 20 years they are currently rated to last. This is important when younger patients who are years away from being considered elderly have a total knee replacement, they will typically need another artificial knee implanted at a later date since they are likely to outlive the implant, which doesn’t always happen with elderly patients.
A diagnosis of sarcoidosis is established on the basis of compatible clinical and radiologic findings and histologic evidence of the presence of noncaseous epithelioid cell granulomas in one or more organs and the absence of causative organisms or particulates (16). Granulomas of known causes and local sarcoidlike reactions must be excluded. Granulomatous lesions may result from many conditions, including tuberculosis, berylliosis, leprosy, hypersensitivity pneumonitis, Crohn disease, primary biliary cirrhosis, and fungal disease. Moreover, local sarcoidlike reactions may be seen in lymph nodes that drain a neoplasm or a site of chronic inflammation (19). Such reactions also have been seen in patients who have undergone chemotherapy and radiation therapy (23). If biopsy of lymph nodes or pulmonary or pleural tissue is necessary for diagnosis, one of three techniques may be used: transbronchial biopsy, CT-guided biopsy, or surgical biopsy (24). The use of a surgical technique may be warranted when the results of biopsy with another procedure are not definitive and biopsy of mediastinal lymph nodes, lung, or both is required. This can generally be done with minimally invasive procedures, such as cervical mediastinoscopy, the Chamberlain procedure (a parasternal minithoracotomy for biopsy of the aortopulmonary window or para-aortic nodes), or video-assisted thoracoscopic surgical biopsy (25).

A rotator cuff tear is a common injury, especially in sports like baseball or tennis, or in jobs like painting or cleaning windows. It usually happens over time from normal wear and tear, or if you repeat the same arm motion over and over. But it also can happen suddenly if you fall on your arm or lift something heavy. Your rotator cuff is a group of four muscles and tendons that stabilize your shoulder joint and let you lift and rotate your arms. There are two kinds of rotator cuff tears. A partial tear is when the tendon that protects the top of your shoulder is frayed or damaged. The other is a complete tear. That’s one that goes all the way through the tendon or pulls the tendon off the bone.
Arteriosclerosis occurs when the blood vessels that carry oxygen and nutrients from your heart to the rest of your body (arteries) become thick and stiff — sometimes restricting blood flow to your organs and tissues. Healthy arteries are flexible and elastic, but over time, the walls in your arteries can harden, a condition commonly called hardening of the arteries. Atherosclerosis is a specific type of arteriosclerosis, but the terms are sometimes used interchangeably. Atherosclerosis refers to the buildup of fats, cholesterol and other substances in and on your artery walls (plaques), which can restrict blood flow. These plaques can burst, triggering a blood clot. Although atherosclerosis is often considered a heart problem, it can affect arteries anywhere in your body. Atherosclerosis may be preventable and is treatable.

Wet dreams occur when you ejaculate during your sleep. The medical term for a wet dream is “nocturnal emission.“ Most wet dreams are reported in teenage boys and young men, and sometimes they occur well into adulthood.
IVC filter is placed to prevent fatal Pulmonary Embolism due to Deep Venous Thrombosis (DVT). This particular patient had extensive DVT of Ilio-Femoral veins leading to massive swelling of left lower limb. The IVC filter was inserted via the Right Femoral Vein. This case was the first IVC filter placement of North Bengal and adjoining areas.
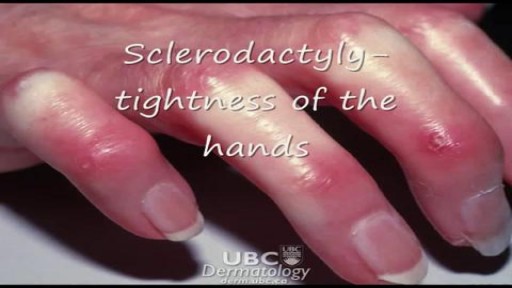
Scleroderma and systemic sclerosis

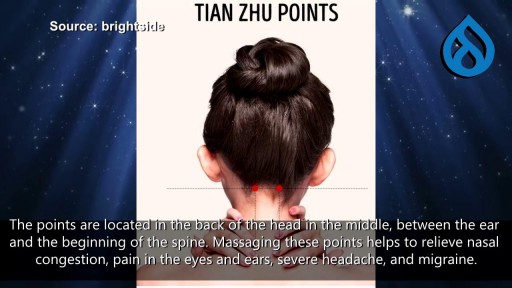
A sneeze, or sternutation, is a semi-autonomous, convulsive expulsion of air from the lungs through the nose and mouth, usually caused by foreign particles irritating the nasal mucosa
Joint Replacement Surgery is part of Orthopedics hence surgical as well as non-surgical techniques are carried out by orthopedic surgeons. The burden of pain can be reduced with the help of minimally invasive orthopedic therapies prescribed by doctors. https://goo.gl/VhzaUr
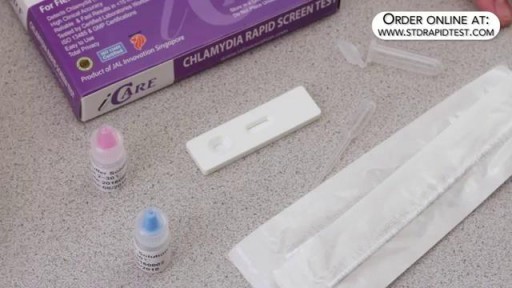
How to use a Chlamydia rapid test kit for self-diagnosis of Chlamydia (swab test). Convenient, Easy to Use, and over 95% Accurate. Certified GMP and ISO13485. Test yourself at home with Complete Privacy. Buy online today at: http://www.stdrapidtest.com

Closure of a loop ileostomy is a relatively simple procedure although many studies have demonstrated high morbidity rates following it. Methods to reduce the number of complications, such as timing of closure or different surgical closure techniques, are investigated. The aim of this study was to evaluate the experience of the Abdominal Surgery Center at Vilnius University Hospital (VUH) ‘Santariskiu klinikos’ to review the complications after closure of loop ileostomy and to identify potential risk factors for postoperative complications.

Watch that video of Removal of a large epidermal cyst in the chest

We get excited when people graduate! May it be graduating from physiotherapy or even graduating onto a new progression of an exercise! Today you move onto new challenges as Mike & Tyler demonstrate the final side plank progression. Kitchener Massage Therapy - http://www.strivept.ca/massage-therapy-kitchener.html
Forzest is the erectile dysfunction tablet meant for treating mens ED disorder, it is approved by FDA and comes in strenght dose 20mg. For more information kindly visit to http://www.medstorerx.com/forzest.aspx

» A kidney stone, also known as a renal calculus (from the Latin rēnēs, “kidneys,” and calculus, “pebble”), is a solid concretion or crystal aggregation formed in the kidneys from dietary minerals in the urine. » Urolithiasis (UL) is one of the most common diseases, with approximately 7.6% incidence in Western India. Although most patients have only one stone episode, 25% of patients experience recurrent stone formation. UL therefore has a significant impact on quality of life and socioeconomic factors.
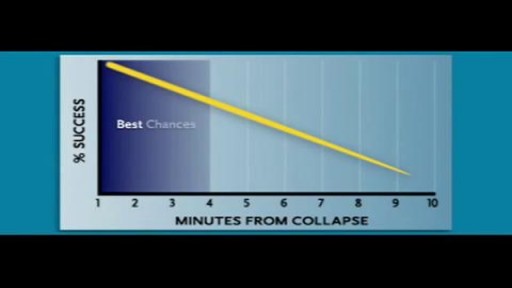
Cardiac arrest usually results from an electrical disturbance in the heart. It's not the same as a heart attack. The main symptom is loss of consciousness and unresponsiveness. This medical emergency needs immediate CPR or use of a defibrillator. Hospital care includes drugs, an implantable device, or other procedures.

Pathology: Previous spinal cord injury, diabetes, renal failure, dynamic knee contracture, open left ankle disarticulation for sepsis and severe foot infection

Treating Lymphedema -
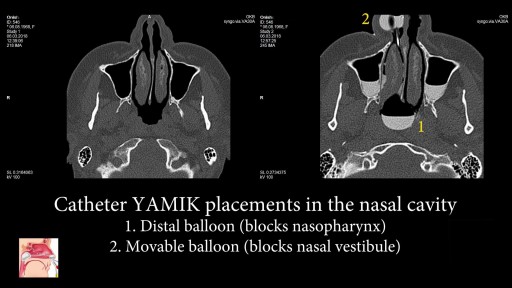
Nasal catheter YAMIK - is a new drug delivery sistem for topical treatment for sinusitis. The introduction of a large volume of the #drugsolution directly into all the paranasal #sinuses - provides new opportunities in the #treatment of #sinusitis! #YamikprocedureNasal catheter YAMIK is a new device for topical sinonasal delivery of medication during rhinosinusitis treatment. Administration of therapeutic solution with YAMIK catheter is called YAMIK procedure. The following features differs YAMIK procedure from all other topical sinonasal delivery techniques: - Medication is delivered into the all paranasal sinuses at one side of nose regardless of their involvement in the inflammatory disease. -Specific position of patient’s head. Patient should lay on the side of of the sinuses, into which solution will be administered. This position is physiological and comfortable for patients, including children and elders. The LHL position was suggested to be the most favorable position for patients to adopt - Therapeutic solutions reliably penetrates into without previous sinus surgery sinuses with natural ostia size. - Paranasal sinuses are filling with medicinal solution by gravity. To accelerate process, it is used small pressure gradient, which created by motion of syringe plunger with amplitude 1 - 2 ml during administration of solution. - It is provided contact of the whole sino-nasal mucosa with medication. - Prolonged time of the contact of sino-nasal mucosa with medicine provides administration of the therapeutically significant dose. Therapeutic solution administered into paranasal sinuses is considered as a STORE. Thanks to affect mucociliary clearance, therapeutic solution is gradually evacuated from sinuses through ostia. Thereby, prolonged nasal irrigation is performed. - Due to extended contact with saline (NaCl 0,9%), viscous colloidal pathological substance filling paranasal sinuses is dissolved. As a result, its viscosity decreases, and substance is removing by mucociliary clearance. Thereby, drainage function of the ostia are returned some time after finish YAMIK method procedure. -The procedure is performing under local anesthesia. - There is no need in active involvement of the patient. Blowing, pronouncing any sounds like “cuckoo”, holding any things and so on is unnecessary. If is performed by a qualified medical professional the procedure is more effective. - Medication contacts only with nasal passages and paranasal sinuses. Thus, it is provided topical drug therapy. - YAMIK procedure is call sinonasal delivery techniques of a therapeutic solution. It differs from nasal techniques, because medicinal solution contacts not only with nasal mucosa, but with mucous membrane of paranasal sinuses. - The only used drug formulation is a solution. - It is possible non-invasive sample extraction from mucosa of paranasal sinuses (for bacteriological, immunological, cytological and a number of others investigation methods).
