- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Of course, these vocal cords are not mine, because I am the one who captured this video before I performed surgery for the patient. See how the cords are normal and freely mobile. Talkative persons have something else....imagine
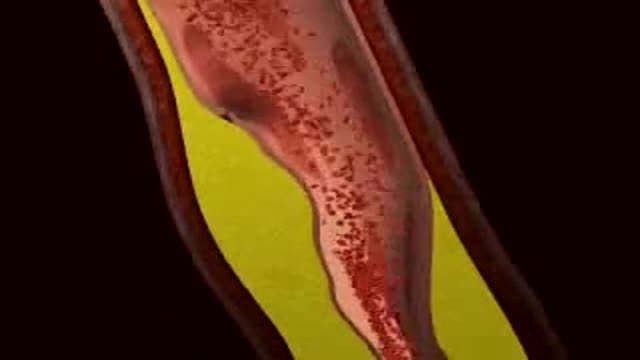
Myocardial Infarction 3D Animation

Special Anoscope for Easy Purse string Suture Application in Stapled Hemorrhoidopexy

Mode of action of NNRTIs

In the Womb - Identical Twins

Wound-closure technologies are becoming less painful and more efficient at closing wounds

What is hemodiafiltration? Hemodiafiltration, or HDF, is a renal replacement modality that combines diffusion and convection to improve removal of molecules in the middle molecular weight range versus hemodialysis.
Find our full video library only on Osmosis Prime: http://osms.it/more.
Join over 3 million current & future clinicians who learn by Osmosis, and over 130 universities around the world who partner with us to make medical and health education more engaging and efficient. We have unparalleled tools and materials to prepare you to succeed in school, on board exams, and as a future clinician. Sign up for a free trial at http://osms.it/more. If you're interested in exploring an institutional partnership, visit osmosis.org/educators to request a personalized demo.
Follow us on social:
Facebook: http://osms.it/facebook
Twitter: http://osms.it/twitter
Instagram for med: http://osms.it/instagram
Instagram for nursing: https://osms.it/ignursing
Linkedin: https://osms.it/linkedin
Our Vision: Everyone who cares for someone will learn by Osmosis.
Our Mission: To empower the world’s clinicians and caregivers with the best learning experience possible. Learn more here: http://osms.it/mission
Medical disclaimer: Knowledge Diffusion Inc (DBA Osmosis) does not provide medical advice. Osmosis and the content available on Osmosis's properties (Osmosis.org, YouTube, and other channels) do not provide a diagnosis or other recommendation for treatment and are not a substitute for the professional judgment of a healthcare professional in diagnosis and treatment of any person or animal. The determination of the need for medical services and the types of healthcare to be provided to a patient are decisions that should be made only by a physician or other licensed health care provider. Always seek the advice of a physician or other qualified healthcare provider with any questions you have regarding a medical condition. © 2023 Elsevier. All rights reserved.

Shaken baby syndrome symptoms and signs include: Extreme irritability Difficulty staying awake Breathing problems Poor eating Tremors Vomiting Pale or bluish skin Seizures Paralysis Coma Other injuries that may not be initially noticeable include bleeding in the brain and eye, damage to the spinal cord and neck and fractures of the ribs, skull and bones. Evidence of prior child abuse also is common.

Try these tips from top fertility experts to increase the odds you'll be prego ASAP…that is, if you want to be. Take Prenatal Vitamins. ... Try to Time It. ... Skip the Lube. ... Cut Back on Caffeine. ... Don't Increase Your Exercise Routine. ... Go Easy on the Alcohol. ... Try to Chill Out.

10 Biggest Babies Ever Born
Epididymitis is infection or less frequently, inflammation of the epididymis (the coiled tube on the back of the testicle). The majority of men that develop epididymitis develop it because of a bacterial infection. Although males of any age can develop epididymitis, it occurs most frequently between ages of 20 to 39.
Wash your hands thoroughly with soap and water before and after treating the wound. Wash the area with mild soap and running water to reduce the risk of infection. Pat dry. Apply antibiotic ointment and cover with a clean bandage or sterile dressing. Antibiotic prophylaxis should be considered, especially if there is a high risk of infection, such as with cat bites, with puncture wounds, with wounds to the hand, and in persons who are immunosuppressed. Amoxicillin/clavulanate is the first-line prophylactic antibiotic.
During surgery to repair the hernia, the bulging tissue is pushed back in. Your abdominal wall is strengthened and supported with sutures (stitches), and sometimes mesh. This repair can be done with open or laparoscopic surgery. You and your surgeon can discuss which type of surgery is right for you.
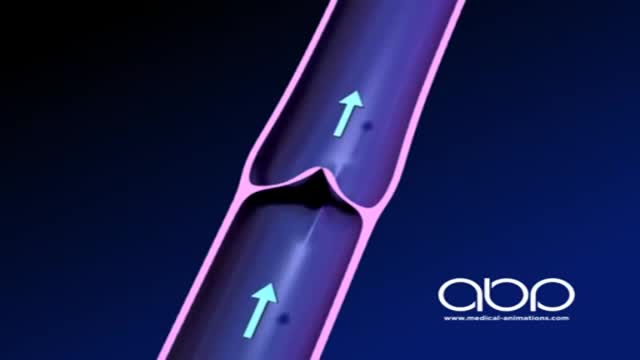
The deep veins play a significant role in propelling blood toward the heart. The one-way valves in deep veins prevent blood from flowing backward, and the muscles surrounding the deep veins compress them, helping force the blood toward the heart, just as squeezing a toothpaste tube ejects toothpaste.

A wisdom tooth or third molar is one of the three molars per quadrant of the human dentition. It is the most posterior of the three. Wisdom teeth generally erupt between the ages of 17

Watch that Hemorrhoids Surgical Repairing Medical Operation

Surgical drainage of dental abscess extending Into the Sub mandibular Space

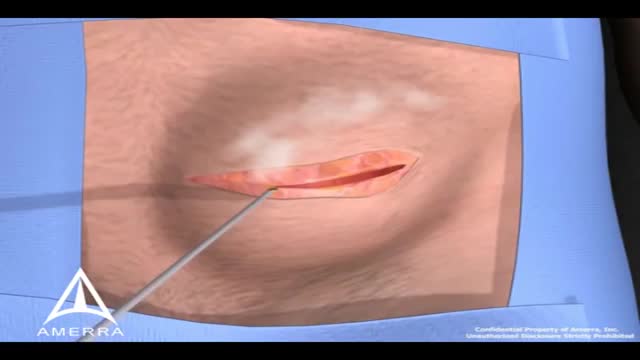
A nonsurgical method of treating a ganglion is to drain the fluid from (aspirate) the ganglion sac. Your doctor can do this in the office using the following procedure: The ganglion area is cleaned with an antiseptic solution. A local anesthetic is injected into the ganglion area to numb the area. When the area is numb, the ganglion sac is punctured with a sterile needle. The fluid is drawn out of the ganglion sac. The ganglion collapses. A bandage and, in some cases, a splint are used for a few days to limit movement and prevent the ganglion sac from filling again. Treating a ganglion by draining the fluid with a needle may not work because the ganglion sac remains intact and can fill again, causing the ganglion to return. For this reason, your doctor may puncture the sac with the needle 3 or 4 times so the sac will collapse completely. Even then, the ganglion is likely to come back.
Hepatitis and chronic alcohol abuse are frequent causes. Liver damage caused by cirrhosis can't be undone, but further damage can be limited. Initially patients may experience fatigue, weakness, and weight loss. During later stages, patients may develop jaundice (yellowing of the skin), gastrointestinal bleeding, abdominal swelling, and confusion. Treatments focus on the underlying cause. In advanced cases, a liver transplant may be needed.
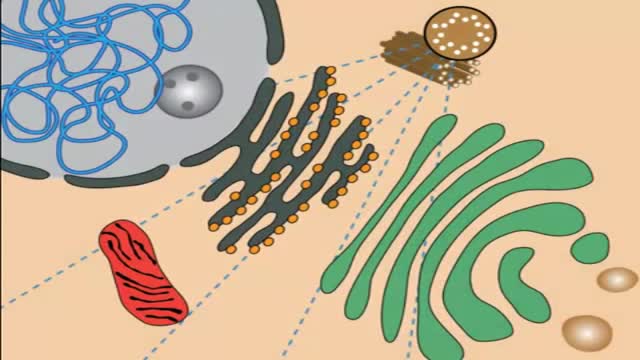
Lysosomal storage diseases (LSDs; /ˌlaɪsəˈsoʊməl/) are a group of approximately 50 rare inherited metabolic disorders that result from defects in lysosomal function. Lysosomes are sacs of enzymes within cells that digest large molecules and pass the fragments on to other parts of the cell for recycling.
