- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Simple technique to harvest Connective tissue graft from the Palate.

This new blood test can help detect and locate cancer
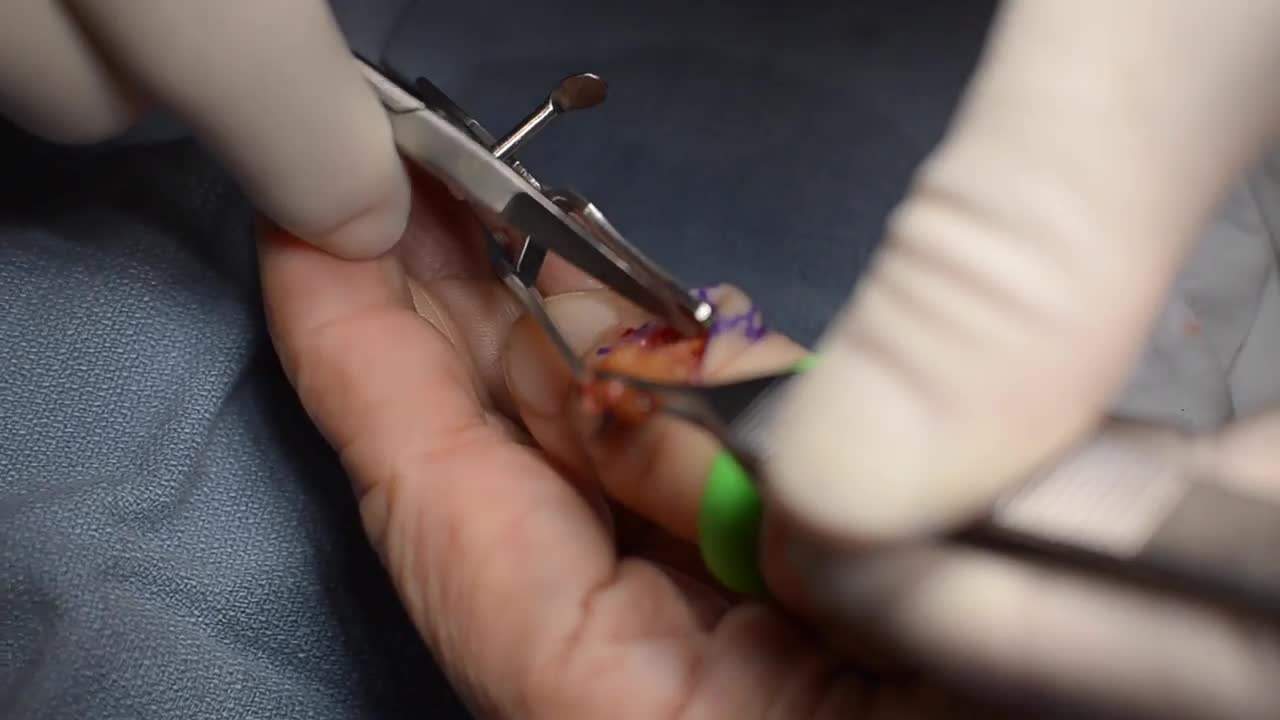
GIANT CELL TUMOR REMOVAL Plastic, Cosmetic and Reconstructive
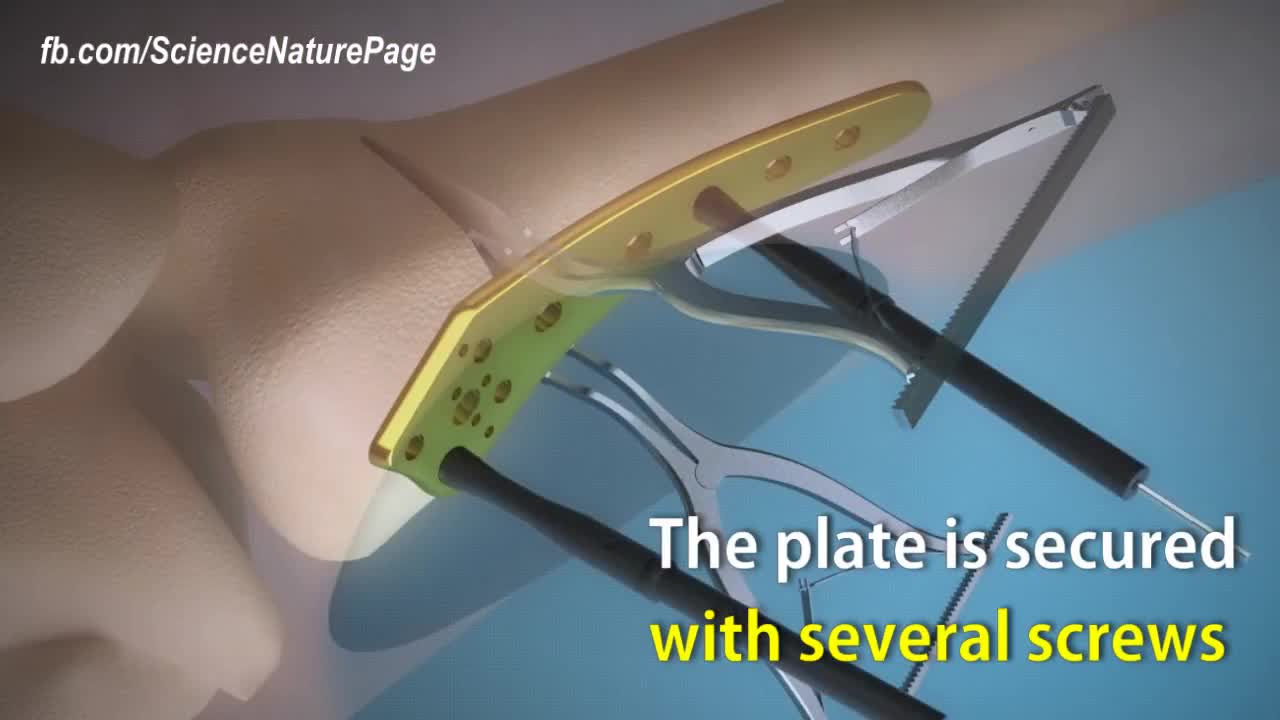
Here is how surgeons perform knock knee correction surgery. Titanium plate is used to stabilize the affected area. The femur is cut nearly through to help with the stability. Spreaders angle the cut align the leg. The plate is secured with several screws. Synthetic bone graft material is packed in the joint. The patient will be in crutches for 4 to 6 weeks.
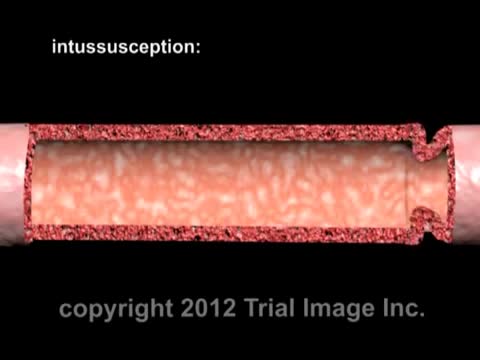
Intussusception (in-tuh-suh-SEP-shun) is a serious condition in which part of the intestine slides into an adjacent part of the intestine. This "telescoping" often blocks food or fluid from passing through. Intussusception also cuts off the blood supply to the part of the intestine that's affected, which can lead to a tear in the bowel (perforation), infection and death of bowel tissue.

3D Printed Models Used in the Mayo Clinic's First Face Transplant
Frontotemporal dementia (frontotemporal lobar degeneration) is an umbrella term for a diverse group of uncommon disorders that primarily affect the frontal and temporal lobes of the brain — the areas generally associated with personality, behavior and language. In frontotemporal dementia, portions of these lobes shrink (atrophy). Signs and symptoms vary, depending upon the portion of the brain affected. Some people with frontotemporal dementia undergo dramatic changes in their personality and become socially inappropriate, impulsive or emotionally indifferent, while others lose the ability to use language.

The brain is the most complex organ in our body. It controls everything we do, from simple things such as breathing, to complex things such as co-ordinating our movements. The brain stores our memories, allows us to think and speak, and controls how we behave
TRANSUMBILICAL SINGLE SITE LAP CHOLYCYSTECTOMY
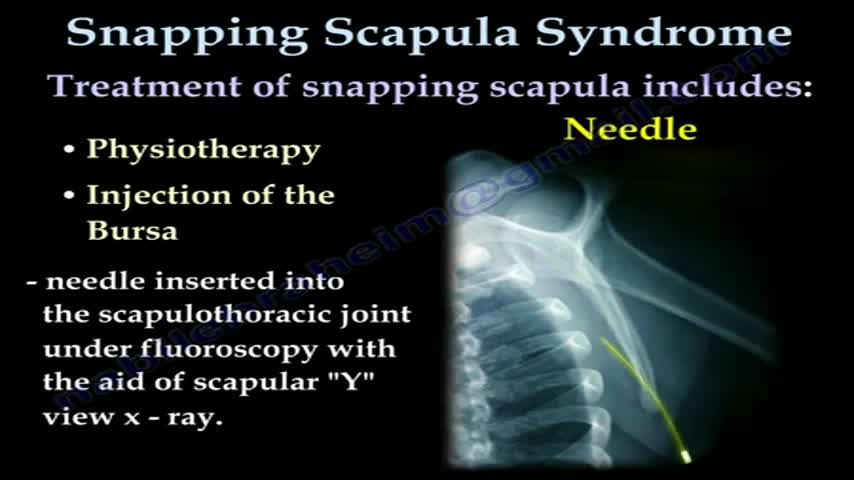
... Orthopedics & Sports Medicine Our Services Where Does it Hurt? SNAPPING SCAPULA SYNDROME PDF Icon PRINTABLE BOOKLET A PATIENT'S GUIDE TO SNAPPING SCAPULA SYNDROME INTRODUCTION The scapulothoracic joint is located where the shoulder blade (also called the scapula) glides along the chest wall (the thorax). When movement of this joint causes feelings or sounds of grating, grinding, popping, or thumping, doctors call it snapping scapula syndrome. Snapping scapula syndrome is fairly rare. When it happens, the soft tissues between the scapula and the chest wall are thick, irritated, or inflamed. Snapping scapula syndrome can also happen if the bones of the shoulder blade or rib cage grate over one another. This guide will help you understand what causes snapping scapula syndrome how doctors treat this condition ANATOMY What parts of the body are involved in this condition? The shoulder is made up of three bones: the humerus (upper arm bone), the clavicle (collarbone), and the scapula(shoulder blade). Two large muscles attach to the front part of the scapula where it rests against the chest wall. One of them, called the subscapularis muscle, attaches over the front of the scapula where it faces the chest wall. The serratus anterior muscle attaches along the edge of the scapula nearest the spine. It passes in front of the scapula, wraps around the chest wall, and connects to the ribs on the front part of the chest. A bursa is a fluid-filled sac that cushions body tissues from friction. A bursa sits between the two muscles of the scapula. There is also a bursa in the space between the serratus anterior muscle and the chest wall. When bursa sacs become inflamed, the condition is called bursitis. Scapulothoracic bursitis refers to inflammation in the bursa under the shoulder blade. This type of bursitis is most common in the upper corner of the scapula nearest the spine. It also occurs under the lower tip of the scapula. In either case, it can cause the sounds and sensations of snapping scapula syndrome. A person can have bursitis in the joint without any grinding or popping. Related Document: A Patient's Guide to Shoulder Anatomy CAUSES What causes this condition? Snapping scapula is caused by problems in the soft tissues or bones of the scapula and chest wall. It can start when the tissues between the scapula and shoulder blade thicken from inflammation. The inflammation is usually caused by repetitive movements. Certain motions of the shoulder done over and over again, such as the movements of pitching baseballs or hanging wallpaper, can cause the tissues of the joint to become inflamed. In other cases, the muscles under the scapula have shrunk (atrophied) from weakness or inactivity. The scapula bone then rides more closely to the rib cage. This means the scapula bumps or rubs on the rib bones during movement. Changes in the alignment or contour of the bones of the scapulothoracic joint can also cause snapping scapula. When a fractured rib or scapula isn't lined up just right, it can cause a bumpy ridge that produces the characteristic grind or snap as the scapula moves over the chest wall.

A rotator cuff tear is a common injury, especially in sports like baseball or tennis, or in jobs like painting or cleaning windows. It usually happens over time from normal wear and tear, or if you repeat the same arm motion over and over. But it also can happen suddenly if you fall on your arm or lift something heavy. Your rotator cuff is a group of four muscles and tendons that stabilize your shoulder joint and let you lift and rotate your arms. There are two kinds of rotator cuff tears. A partial tear is when the tendon that protects the top of your shoulder is frayed or damaged. The other is a complete tear. That’s one that goes all the way through the tendon or pulls the tendon off the bone.

There is nothing that compares to the fresh-faced feeling you have when you leave the aesthetician after a facial. There is just something so freeing about knowing that nasty little buggers like blackheads, whiteheads and all other kinds of heads have been given the heave-ho. That could be why this Facebook video of a blackhead being removed has gone viral. With more than 24 million views, the popular video is weirdly difficult to stop watching.
Glioblastoma is a type of astrocytoma, a cancer that forms from star-shaped cells in the brain called astrocytes. In adults, this cancer usually starts in the cerebrum, the largest part of your brain

Exam- COPD Patient

This membrane could prevent heart attacks and keep the heart alive.

Skin grafting is a surgical procedure that involves removing the skin from one area of the body and moving it, or transplanting it, to a different area of the body. This surgery may be done if a part of your body has lost its protective covering of skin due to burns, injury, or illness. Skin grafts are performed in a hospital. Most skin grafts are done using general anesthesia, which means you’ll be asleep throughout the procedure and won’t feel any pain.

A knee revision, from Pakistan!!

Home > Baby > Breastfeeding > Top 10 Tips for Boosting Your Breast Milk Supply Top 10 Tips for Boosting Your Breast Milk Supply COMMENTS () | PRINT A nursing mom’s biggest worry is whether or not she’s making enough milk. We’ve gathered 10 tips to help you bump up your milk production. This gallery is not intended to substitute medical advice. If you have any concerns, contact a lactation consultant or your healthcare provider immediately. 1. Nurse, Nurse, Nurse Breasts work on demand. The more your little one nurses, the more milk your body will create. When your little one is going through a growth spurt, it’s easy to fall into thinking, “my baby is so hungry I must not have enough milk.” What’s really happening is your baby is priming your body to have enough milk to support how big your baby will be after the spurt. The worst thing for your supply is to supplement with formula during a growth spurt. It can be hard to devote most of your day to nursing, but it’s the best thing for your baby, and your supply.

Many mothers notice engorgement, or over-filled breasts, at some point or the other while they are breast-feeding their baby and it is especially common to experience when your baby is first born and you are just starting to make milk. So for the first couple of days you make colostrum and then 2-5 days later your milk comes in. And sometimes it comes in with a vengeance and all of the sudden you feel really full and it can be painful and very uncomfortable. Normally your milk supply will even out and start to work well with your babys demand, so it is kind of a supply and demand type of function, but until then, if you feel engorgement, there are a few things you can do to relieve it. If you are nursing your baby on demand this will usually help to self-regulate and most young babies want to eat every 2-3 hours and sometimes even every hour. So, basically, the more often your breasts are emptied the more relief you will feel. But on the same hand, the more you nurse the more milk your body will probably produce. This is why it is good to go off of your babys cues because then you will make what your baby needs and hopefully not much more. But if you are making more than your baby needs and you find that you are still full after feedings you will probably have to either manually express some milk or pump it off, so have a good pump available in case you need to, and if you don't, you can manually express the milk by gently massaging from the armpit down towards the nipple. And you can also try using heat prior to nursing your baby or pumping milk off and this will also help to relax things and help you to get the milk out. Take a warm shower and then feed your baby or use a warm compress.
Joint Replacement Surgery is part of Orthopedics hence surgical as well as non-surgical techniques are carried out by orthopedic surgeons. The burden of pain can be reduced with the help of minimally invasive orthopedic therapies prescribed by doctors. https://goo.gl/VhzaUr
