- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Diagnose an abusive relationship and you will be on your way to ending domestic abuse. Getting a definitive, objective diagnosis can put you in the "stop-guessing" mode and into the "start-treating" mode in moments.
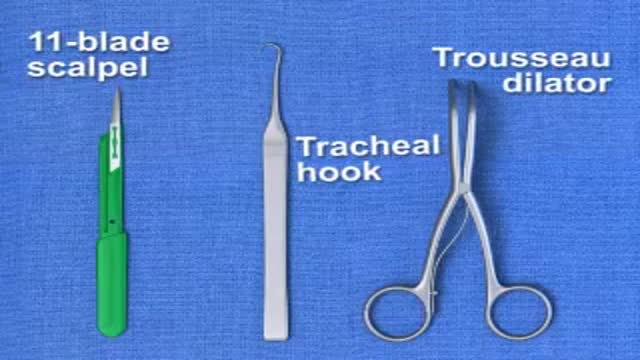
Brief animation demonstrating emergency surgical cricothyrotomy; created with Lightwave 9.3
Preparing Syringes for Injections
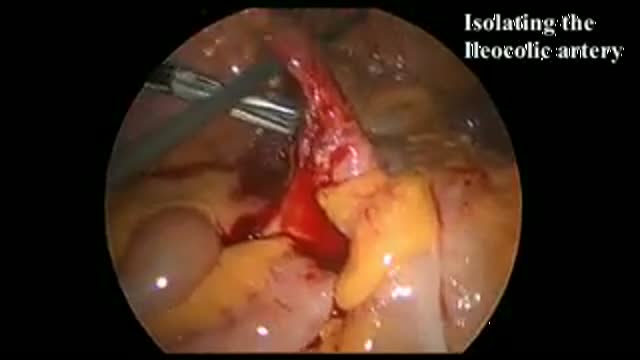
Bleeding during the ligation of an artery during right hemicolectomy

this video is showing the laparoscopic transabdominal preperitoneal herina repair for direct inguinal herina

A video showing thyroidectomy surgery
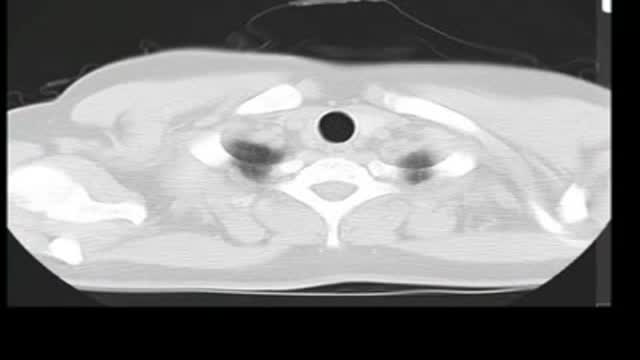
Pulmonary alveolar proteinosis. Please see disclaimer on my website. www.academyofprofessionals.com. MCQs are also available.
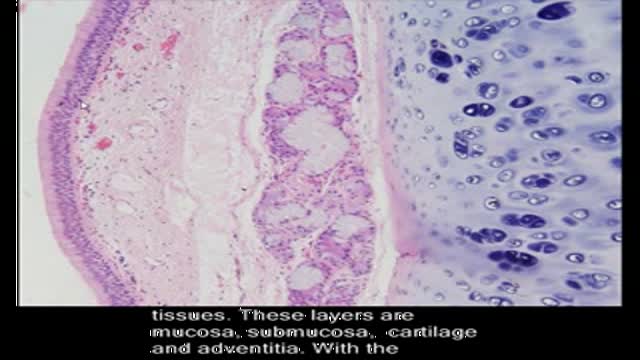
the short video will describe four layers of connective tissue. Please see disclaimer on my website. www.academyofprofessionals.com
Nice surgery video
Breast Reduction Surgery video Operation مركز افارا لجراحات التجميل الخدود تكبير الشفايف
A video showing the procedure of Tubular Diskectomy of a herniated disk. Uploaded on MedicalVideos.us.Discussing the management of Sciatica.
Video of the technique and early outcomes of Robotic Assisted Microsurgical Vasectomy Reversal at University of Florida and Shands, Gainesville, Fl, by Dr. Sijo Parekattil.

Graphic video demonstrating the reconstruction of a facial cheek defect following the removal of a common skin cancer in a challenging location near the lower eyelid. Visit us @ www.skincancercentre.com.

Vocal Cord Surgery HD

Vaginal Hysterectomy using Thermal Hemostasis

Total Knee Replacement Surgery Video
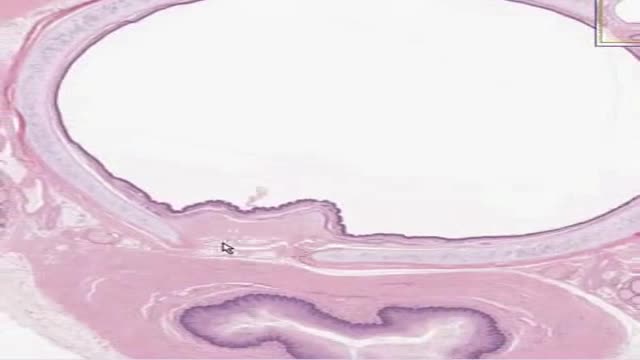
Histology of Trachea

Basic Respiratory Clinical Exam Video
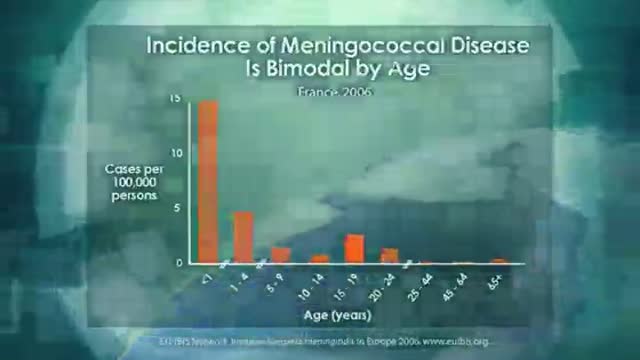
Meningeococcal Bacterial Maningitis Introduction
Baby Delivery
