- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Folic acid, which is also called folate, is a B vitamin. The best food sources of folic acid are fortified cereals. Folic acid plays an important role in the production of red blood cells and helps your baby's neural tube develop into her brain and spinal cord.

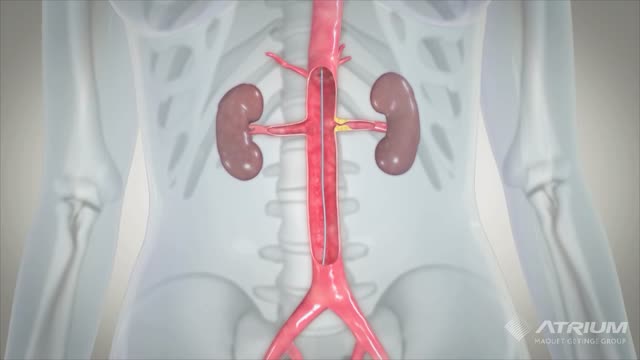
During surgery to repair the hernia, the bulging tissue is pushed back in. Your abdominal wall is strengthened and supported with sutures (stitches), and sometimes mesh. This repair can be done with open or laparoscopic surgery. You and your surgeon can discuss which type of surgery is right for you.

the elbow is the second most frequently dislocated major joint, after the shoulder. It is the most commonly dislocated joint in children. [1] More than 90% of all elbow dislocations are posterior dislocations. This injury entails disengagement of the coronoid process of the ulna from the trochlea of the humerus with movement posteriorly. [2] The mechanism of injury is typically a fall onto an outstretched hand (FOOSH) with the elbow in extension upon impact.
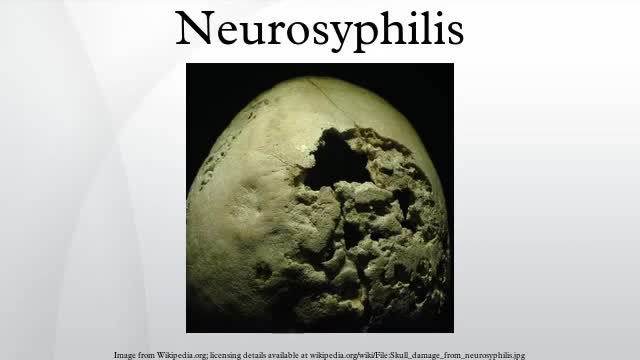
Neurosyphilis is an infection of the brain or spinal cord caused by the spirochete Treponema pallidum. It usually occurs in people who have had chronic, untreated syphilis, usually about 10 to 20 years after first infection and develops in about 25%–40% of persons who are not treated. The United States' Centers for Disease Control and Prevention (CDC) advises that neurosyphilis can occur at any stage of a syphilis infection.

Zinc deficiency symptoms include growth and development problems, hair loss, diarrhea, impotence, eye and skin conditions, and loss of appetite. Other symptoms may include weight loss, delayed wound healing, taste changes, and mental slowness.

Alagille syndrome (AS) is an autosomal dominant disorder (OMIM 118450) associated with abnormalities of the liver, heart, skeleton, eye, and kidneys and a characteristic facial appearance. In 1973, Watson and Miller reported 9 cases of neonatal liver disease with familial pulmonary valvular stenosis.

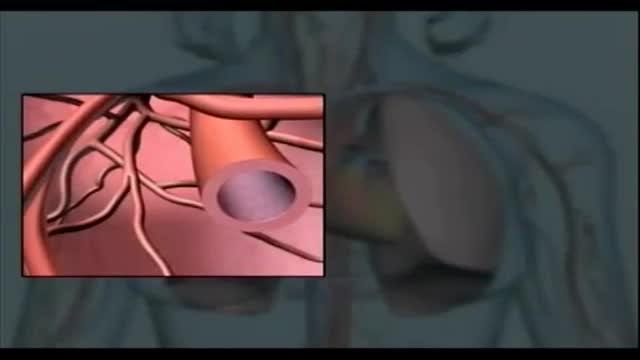
Blood cells travel through the circulatory system suspended in a yellowish fluid called plasma. Plasma is 90% water and contains nutrients, proteins, hormones, and waste products. Whole blood is a mixture of blood cells and plasma.
The urinary bladder is a hollow muscular organ that collects urine from the kidneys before disposal by urination. A hollow muscular, and distensible (or elastic) organ, the bladder sits on the pelvic floor. Urine enters the bladder via the ureters and exits via the urethra.
Anaphylaxis is a severe, potentially life-threatening allergic reaction. It can occur within seconds or minutes of exposure to something you're allergic to, such as a peanut or the venom from a bee sting. The flood of chemicals released by your immune system during anaphylaxis can cause you to go into shock; your blood pressure drops suddenly and your airways narrow, blocking normal breathing. Signs and symptoms of anaphylaxis include a rapid, weak pulse, a skin rash, and nausea and vomiting. Common triggers of anaphylaxis include certain foods, some medications, insect venom and latex. Anaphylaxis requires an immediate trip to the emergency department and an injection of epinephrine. If anaphylaxis isn't treated right away, it can lead to unconsciousness or even death.

Arthritis occurs when the cartilage breaks down explains Dr. Derek Papp, Sports Medicine Physician with Miami Orthopedics & Sports Medicine Institute. This it’s a very common knee injury such as the damage of the cartilage and meniscus tear.
ACL tears is another common injury especially in sports like soccer or Australian football, the specialist explains.
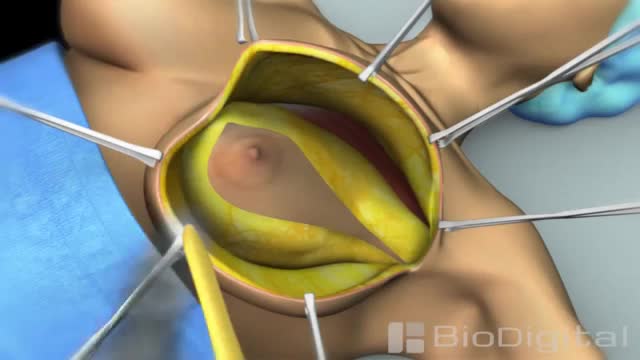
Mastectomy is surgery to remove all breast tissue from a breast as a way to treat or prevent breast cancer. For those with early-stage breast cancer, mastectomy may be one treatment option. Breast-conserving surgery (lumpectomy), in which only the tumor is removed from the breast, may be another option.
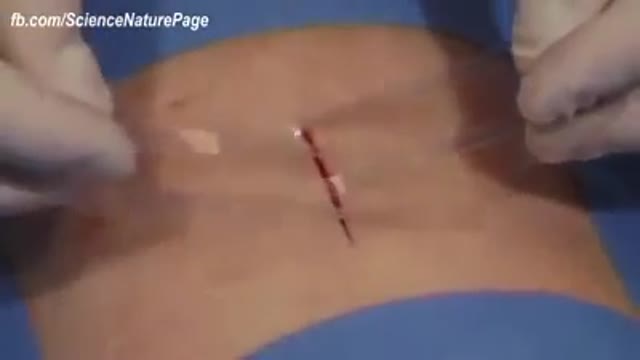
Wound-closure technologies are becoming less painful and more efficient at closing wounds.

Happy New Year 2017

Sever's disease (also known as calcaneal apophysitis) is a type of bone injury in which the growth plate in the lower back of the heel, where the Achilles tendon (the heel cord that attaches to the growth plate) attaches, becomes inflamed and causes pain.

Genes are the building blocks of heredity. They are passed from parent to child. They hold DNA, the instructions for making proteins. Proteins do most of the work in cells. They move molecules from one place to another, build structures, break down toxins, and do many other maintenance jobs. Sometimes there is a mutation, a change in a gene or genes. The mutation changes the gene's instructions for making a protein, so the protein does not work properly or is missing entirely. This can cause a medical condition called a genetic disorder. You can inherit a gene mutation from one or both parents. A mutation can also happen during your lifetime.
A ureteral stent, sometimes as well called ureteric stent, is a thin tube inserted into the ureter to prevent or treat obstruction of the urine flow from the kidney. The length of the stents used in adult patients varies between 24 to 30 cm.

Enchondroma (Cartilage) benign tumor of the finger.
Getting the right diagnosis often isn’t easy for psychiatric conditions. In our field, we don’t yet have biologic tests that can easily define one condition from another. If your blood pressure is 140 over 90, you have hypertension or high blood pressure. In mental health, we have to rely on a description of patterns or symptoms to makes diagnoses. This model is fraught with challenges. Without a clear biological model to work from, and given the complexity of the human brain, the field has settled upon dividing these descriptions of symptoms into syndromes. The Diagnostic and Statistical Manual of Mental
Intestino Irritable Tratamiento, Colon Irritable, Tratamiento Para El Colon Irritable--- http://intestino-irritable-tratamiento.plus101.com --- Si usted está sufriendo de Síndrome del Intestino Irritable SII, aquí hay una serie de técnicas y estrategias que se conocen para aliviar grandemente los síntomas a largo y corto plazo. La alimentación es la fuente de energía primordial que tenemos y es por eso que hay que darle una importancia suprema a la hora de querer atacar los síntomas del SII. Se recomienda el consumo de hierbas, tales como: manzanilla, consuelda, aceite de onagra, bálsamo de limón, hinojo, canela, nuez moscada, cúrcuma, todas las especias y enzimas digestivas. Todas ellas producen grandes beneficios para su organismo, dentro de los cuales destacamos: La manzanilla actúa como carminativo, así como calmante y agente tonificante para el tracto digestivo. Los aceites esenciales de manzanilla también han contribuido a aliviar cólicos intestinales e irritación en los animales. La manzanilla se toma normalmente tres veces al día, entre las comidas, en una forma de té. La consuelda tiene un uso como agente tópico para mejorar la cicatrización de heridas, úlceras en la piel, tromboflebitis y torceduras. También se utiliza para las personas con problemas gastrointestinales, como úlceras de estómago y el síndrome del intestino irritable, y para quienes sufren problemas pulmonares. Una combinación de menta, comino y otras dos hierbas carminativas (para aliviar los gases), semillas de hinojo y ajenjo, han resultado ser un tratamiento eficaz para los dolores abdominales. La acacia tiene un alto contenido de fibra y con frecuencia se recomienda para aliviar la irritabilidad intestinal. Las frutas como la papaya, el plátano, el mango, la piña, las fresas y los arándanos son altamente recomendables. Las verduras como las patatas dulces, la calabaza y las zanahorias no pueden dejar de ser parte de su dieta. Tenga cuidado con algunos de los medicamentos recetados para el SII ya que algunos de ellos han sido retirados del mercado debido a que contenían ingredientes tóxicos. Algunos ingredientes contenidos en medicamentos de venta libre para el resfriado también han demostrado efectos negativos en pacientes con SCI. Recomendamos las gotas de zinc como una alternativa durante un resfriado ya que no irrita el estómago y tiene visibles resultados de estímulo inmunológico. Los alimentos que se deben evitar: lácteos, huevos (especialmente la yema debido al alto contenido de grasa), brócoli, maíz, aceites hidrogenados, jarabe de maíz alto en fructosa, manzanas (debido al alto contenido de fructosa), frijoles, chocolate (debido a la cafeína) , café, té con cafeína. Para obtener más información sobre cómo poder controlar y eliminar los síntomas del SII, puede visitar el sitio http://intestino-irritable-tratamiento.plus101.com

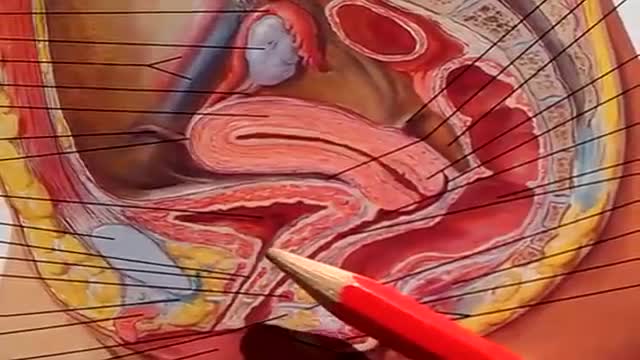
You may have heard that some positions, such as your partner on top (missionary position), are better than others for getting pregnant. In fact, there's no evidence to back these theories up. Experts just haven't done the research yet. What experts have done, though, is use scanning to show what's going on inside when you're doing the deed. The research looked at two positions: the missionary position and doggy style. (Doggy style being when you're on all fours, and your partner enters you from behind). Common sense tells us that these positions allow for deep penetration. This means that they're more likely to place sperm right next to your cervix (the opening of your uterus). The scans confirm that the tip of the penis reaches the areas between the cervix and vaginal walls in both of these positions. The missionary position allows the penis to reach the area at the front of the cervix. The rear entry position reaches the area at back of the cervix. It's amazing what some experts spend their time doing, isn't it! Other positions, such as standing up, or woman on top, may be just as good for getting sperm right next to the cervix. We just don't know yet. http://www.babycentre.co.uk/sex-for-getting-pregnant#ixzz4XKnPLbxL
