- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
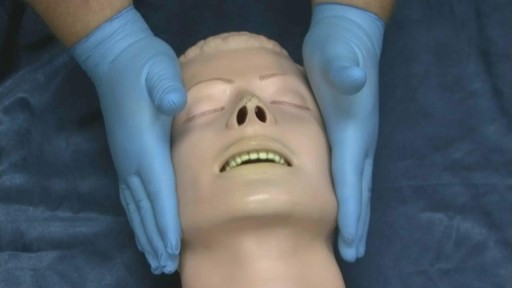
The jaw thrust is a method of opening the airway of a patient. The airway is very important in first aid! It consists of the structures in the back of the throat and upper neck. A patient who is unconscious is not able to maintain their own airway as it can become blocked by the tongue (see picture). Normally, first aid courses teach the head tilt – chin lift technique to open an airway. However, this airway manoeuvre involves significant movement of the patient’s neck. Therefore if there is any suspicion of a spinal (neck) injury it may cause further damage.

An omphalocele is a birth defect in which an infant's intestine or other abdominal organs are outside of the body because of a hole in the belly button (navel) area. The intestines are covered only by a thin layer of tissue and can be easily seen.

NEET Motivational Video |Don't Give up 🔥|#neet2023#aiims
#neetmotivation
#aiims
#neet2023
#pw#dontgiveup
#dream
#mbbs
#neet2024
#doctor
#aiimsdelh#medical

Testosterona En Hombres, Producir Mas Testosterona, Aumentar Deseo Hombre, Baja Testosterona --- http://aumentar-testosterona.good-info.co/ -- ¿Sus testículos son pequeños o se están encogiendo? La atrofia testicular es un enorme problema para los hombres hoy en día, lo sé porque recibo muchos correos electrónicos referentes al tema. Y no solo se ven afectados los hombres más viejos, es francamente aterrador ver cuántos correos electrónicos recibo de hombres jóvenes, y cuando quiero decir jóvenes estoy hablando de hombres de 16, 17 y 18 años de edad. A esta edad sus testículos no deberían encogerse, deberían estar enormes, plenos y pesados de semen, a los 18 años de edad deberían ser una máquina de producir esperma. Pero incluso a los 60 años y más allá, debería estar produciendo una cucharadita de esperma por eyaculación, si no es así tiene trabajo que hacer. Vamos a llegar a la raíz de su problema y a trazar un plan para revertir los testículos que se achican, pero en primer lugar, quiero hablar acerca de los factores del estilo de vida en los hombres jóvenes modernos. Los hombres maduros también necesitan prestar atención a esto, porque mucho de esto también se aplica a ellos. Estos días está de moda ser vegetariano, ingerir mucha hierba de trigo, queso de soya y carbohidratos, se toma leche de soya en lugar de leche entera. Asi mismo, en lugar de comer carne de res alimentada con pasto y salmón salvaje se ingieren hamburguesas de tofu y salchichas de tofu La soya secará sus testículos, en un reciente estudio de la University of Medicine and Dentistry of New Jersey, los científicos probaron polvo de proteína de soya en los hombres y llegaron a la siguiente conclusión: La testosterona sérica disminuyó en un 19% durante las primeras 4 semanas de uso de proteína de soya en polvo y siguió alto durante las 2 semanas posteriores a que descontinuara el consumo de proteína de soya en polvo. aumentar tu virilidad, libido y energia naturalmente haciendo click aqui http://aumentar-testosterona.good-info.co/

Try these tips from top fertility experts to increase the odds you'll be prego ASAP…that is, if you want to be. Take Prenatal Vitamins. ... Try to Time It. ... Skip the Lube. ... Cut Back on Caffeine. ... Don't Increase Your Exercise Routine. ... Go Easy on the Alcohol. ... Try to Chill Out.
Epididymitis is infection or less frequently, inflammation of the epididymis (the coiled tube on the back of the testicle). The majority of men that develop epididymitis develop it because of a bacterial infection. Although males of any age can develop epididymitis, it occurs most frequently between ages of 20 to 39.
Wash your hands thoroughly with soap and water before and after treating the wound. Wash the area with mild soap and running water to reduce the risk of infection. Pat dry. Apply antibiotic ointment and cover with a clean bandage or sterile dressing. Antibiotic prophylaxis should be considered, especially if there is a high risk of infection, such as with cat bites, with puncture wounds, with wounds to the hand, and in persons who are immunosuppressed. Amoxicillin/clavulanate is the first-line prophylactic antibiotic.

Mastitis is an infection of the breast tissue that results in breast pain, swelling, warmth and redness. You also might have fever and chills. Mastitis most commonly affects women who are breast-feeding (lactation mastitis), although sometimes this condition can occur in women who aren't breast-feeding. In most cases, lactation mastitis occurs within the first six to 12 weeks after giving birth (postpartum), but it can happen later during breast-feeding. The condition can cause you to feel run down, making it difficult to care for your baby. Sometimes mastitis leads a mother to wean her baby before she intends to, but continuing to breast-feed, even while taking an antibiotic for the mastitis, is better for you and your baby.
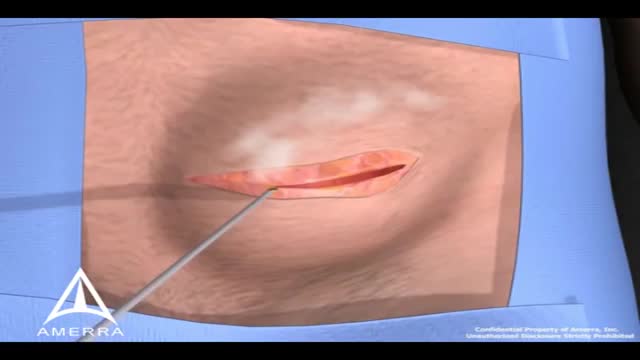
During surgery to repair the hernia, the bulging tissue is pushed back in. Your abdominal wall is strengthened and supported with sutures (stitches), and sometimes mesh. This repair can be done with open or laparoscopic surgery. You and your surgeon can discuss which type of surgery is right for you.
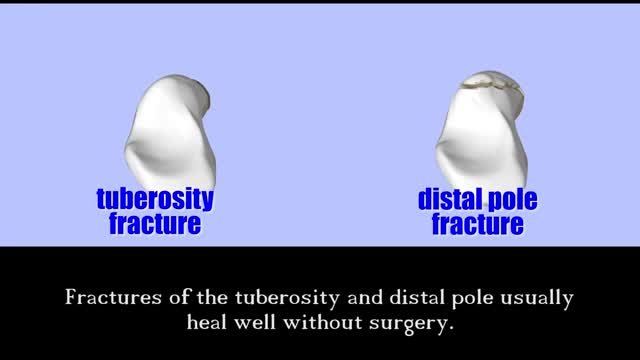
An animated description of the use of a cannulated Herbert screw for surgical treatment of scaphoid fractures.
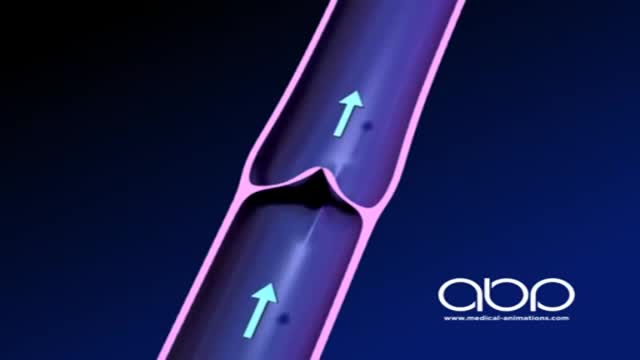
The deep veins play a significant role in propelling blood toward the heart. The one-way valves in deep veins prevent blood from flowing backward, and the muscles surrounding the deep veins compress them, helping force the blood toward the heart, just as squeezing a toothpaste tube ejects toothpaste.
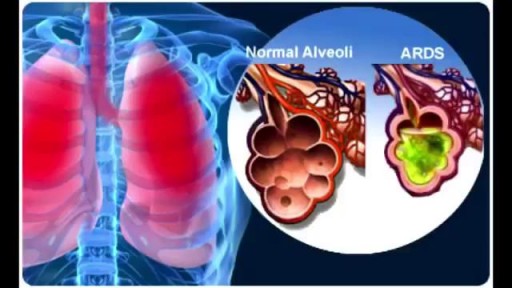
ARDS was recognized as the most severe form of acute lung injury (ALI), a form of diffuse alveolar injury. The AECC defined ARDS as an acute condition characterized by bilateral pulmonary infiltrates and severe hypoxemia in the absence of evidence for cardiogenic pulmonary edema. The severity of hypoxemia necessary to make the diagnosis of ARDS was defined by the ratio of the partial pressure of oxygen in the patient’s arterial blood (PaO2) to the fraction of oxygen in the inspired air (FiO2). ARDS was defined by a PaO2/FiO2 ratio of less than 200, and in ALI, less than 300. This definition was further refined in 2011 by a panel of experts and is termed the Berlin definition of ARDS. [3] ARDS is defined by timing (within 1 wk of clinical insult or onset of respiratory symptoms); radiographic changes (bilateral opacities not fully explained by effusions, consolidation, or atelectasis); origin of edema (not fully explained by cardiac failure or fluid overload); and severity based on the PaO2/FiO2 ratio on 5 cm of continuous positive airway pressure (CPAP). The 3 categories are mild (PaO2/FiO2 200-300), moderate (PaO2/FiO2 100-200), and severe (PaO2/FiO2 ≤100).
Coronary artery bypass grafting (CABG) is a type of surgery that improves blood flow to the heart. Surgeons use CABG to treat people who have severe coronary heart disease (CHD). CHD is a disease in which a waxy substance called plaque (plak) builds up inside the coronary arteries.

A wisdom tooth or third molar is one of the three molars per quadrant of the human dentition. It is the most posterior of the three. Wisdom teeth generally erupt between the ages of 17

In the Womb - Identical Twins
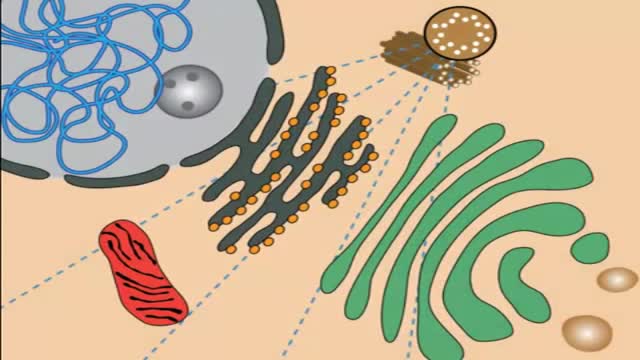
Lysosomal storage diseases (LSDs; /ˌlaɪsəˈsoʊməl/) are a group of approximately 50 rare inherited metabolic disorders that result from defects in lysosomal function. Lysosomes are sacs of enzymes within cells that digest large molecules and pass the fragments on to other parts of the cell for recycling.

Watch that video of A Man Impaled by Shovel Inside His Butt - ER Stories

Medical Terminology

At URBN Dental, we provide you with top oral hygiene tips to help keep your mouth clean, healthy, and happy. Your manual toothbrush usually comes equipped with a tongue cleaner on the back of its head. That can be helpful in scrubbing your tongue, or you can also use a tongue cleaner. By using simple forward motions on the tongue, you can rid the area of plaque and bacteria which often cause bad breath, gingivitis, and harmful mouth ulcers.
The vast majority of glucocorticoid activity in most mammals is from cortisol, also known as hydrocortisone. Corticosterone, the major glucocorticoid in rodents, is another glucocorticoid. Cortisol binds to the glucocorticoid receptor in the cytoplasm and the hormone-receptor complex is then translocated into the nucleus, where it binds to its DNA response element and modulates transcription from a battery of genes, leading to changes in the cell's phenotype. Only about 10% of circulating cortisol is free. The remaining majority circulates bound to plasma proteins, particularly corticosteroid-binding globulin (transcortin). This protein binding likely decreases the metabolic clearance rate of glucocorticoids and, because the bound steroid is not biologically active, tends to act as a buffer and blunt wild fluctuations in cortisol concentration.
