- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

GIANT EAR WAX REMOVAL By using the elephant ear device.It's very useful video for medical students.Please share it!

Ultrasound or ultrasonography is a medical imaging technique that uses high frequency sound waves and their echoes. The technique is similar to the echolocation used by bats, whales and dolphins, as well as SONAR used by submarines. In ultrasound, the following events happen: The ultrasound machine transmits high-frequency (1 to 5 megahertz) sound pulses into your body using a probe. The sound waves travel into your body and hit a boundary between tissues (e.g. between fluid and soft tissue, soft tissue and bone). Some of the sound waves get reflected back to the probe, while some travel on further until they reach another boundary and get reflected. The reflected waves are picked up by the probe and relayed to the machine. The machine calculates the distance from the probe to the tissue or organ (boundaries) using the speed of sound in tissue (5,005 ft/s or1,540 m/s) and the time of the each echo's return (usually on the order of millionths of a second). The machine displays the distances and intensities of the echoes on the screen, forming a two dimensional image like the one shown below.

Oral therapy has potential for symptom relief. It has the advantage of no surgery. Disadvantages include ongoing medication therapy, risks of side effects, high out of pocket cost, and sometimes over time effectiveness diminishes. Certain men also do not like to take medications. This is the most common way to treat BPH. Medicines like Flomax, Cardura, Hytrin and Uroxatral have proven to be effective in the treatment of most cases. Alpha Blockers relieve the obstruction by trying to stop the process by which the construction occurs. They basically relax the smooth muscle cells in the prostate to relieve urinary obstruction. Like most medicines side effects can occur. They are mild in most cases and include dizziness on standing, feeling fatigued, loss of ability to ejaculate with orgasm.
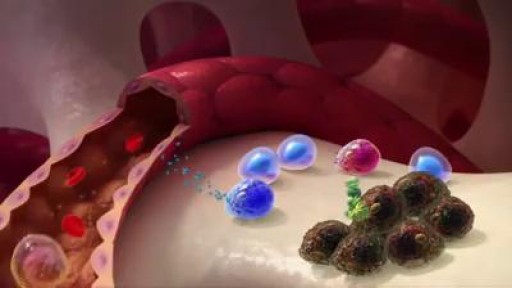
Multiple myeloma is a cancer formed by malignant plasma cells. Normal plasma cells are found in the bone marrow and are an important part of the immune system.

A boxer's fracture is a break through the bones of the hand that form the knuckles. Some doctors use the term "brawler's fracture" rather than "boxer's fracture" because a boxer is not likely to get this injury. The less well-trained brawlers have to learn how to punch without hurting themselves. The metacarpal bones in the hand connect the bones in the finger to the bones in the wrist. There are five metacarpal bones, one to connect each finger to the wrist. All of the metacarpal bones have the same anatomic structure. Each consists of the base, the shaft, the neck, and the head
A foot of gauze out of nipple abscess

Art restoration of anterior teeth

Simply put, there isn’t enough room for wisdom teeth because our jaws don’t grow to be big enough to have enough space for them to come in. Since there isn’t enough room for them to erupt properly, wisdom teeth tend to come in at an angle or they don’t fully emerge, which causes problems for the rest of the mouth. Third molars (the wisdom teeth) routinely damage the teeth right next door, called second molars. Dentists recommend removing wisdom teeth before they become a problem and to avoid a more complicated surgery. Read more at Ask the Dentist: https://askthedentist.com/wisdom-teeth-removal/

Watch that video of 82 Years Old Woman Pregnant For 40 Years

Watch that video to know How To Whiten Your Yellow Teeth Naturally

Watch that video to know How Hot Dogs are Made

Watch that video of an Ingrown Hair Causes Huge Tumor in a Man's Stomach

Hip dysplasia is the medical term for a hip socket that doesn't fully cover the ball portion of the upper thighbone. This allows the hip joint to become partially or completely dislocated

The goal of breast cancer surgery is to remove the entire tumor from the breast. Some of the lymph nodes in the underarm area (axillary nodes) may also be removed to see if cancer cells are present.
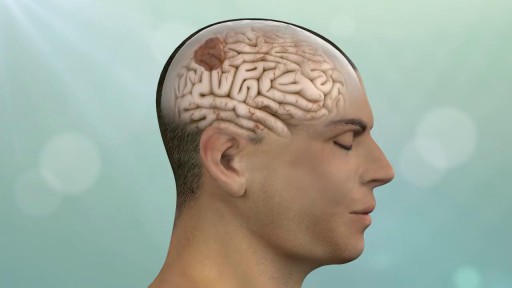
Keyhole surgery can be helpful for patients with brain, pituitary and skull base tumors. With cutting edge technology and a proven track record in keyhole and endonasal endoscopic approaches, we make surgery safer, less invasive and more effective.

How Did Insects Evolve To Feast On Your Blood?

Unstable ankle joints after internal fixation of type B malleolar fractures exist. Residual instability most often occurs after trimalleolar fractures with initial joint dislocation. Treatment with an additional positioning screw generally produced a satisfactory result.

Robotic Surgery Demonstration Using Da Vinci Surgical System
this animated surgery showing management of bone defects with the Precice Lengthening-Compression IM nail

