- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
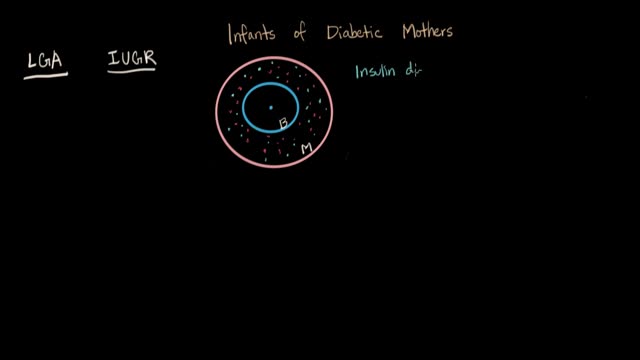
Because the continuous supply of glucose is stopped after birth, the neonate develops hypoglycemia because of insufficient substrate. Stimulation of fetal insulin release by maternal hyperglycemia during labor significantly increases the risk of early hypoglycemia in these infants.

Classical PKU is an autosomal recessive disorder, caused by mutations in both alleles of the gene for phenylalanine hydroxylase (PAH), found on chromosome 12. In the body, phenylalanine hydroxylase converts the amino acid phenylalanine to tyrosine, another amino acid.
Your body needs bile, but if it has too much cholesterol in it, that makes gallstones more likely. It can also happen if your gallbladder can't empty properly. Pigment stones are more common in people with certain medical conditions, such as cirrhosis (a liver disease) or blood diseases such as sickle cell anemia.

Developmental Milestones: Baby Talk from First Sounds to First Words

Frontotemporal degeneration (FTD) is a disease process that results in progressive damage to the temporal and/or frontal lobes of the brain. It causes a group of brain disorders that share many clinical features.

Our results in this study of MIPO treated with conventional plates are comparable to the results of the femoral shaft fractures treated with intramedullary nailing. The technique can be used for all femoral shaft fractures. Although the biomechanics of the plate fixation are less stable compared to the intamedullary nail, the mechanical stability is stable enough for bone healing. Healing was rapid, and postoperative care was simplified. The two major complications were malalignment and screw breakage. We recommend using at least three separated screws in each fragment to prevent stress on the screw and screw breakage. Intraoperative limb length, axial alignment, and rotation must be carefully assessed to prevent malalignment. The limitations of our study include lack of a comparison group, retrospective data collection, and no randomisation in outcome evaluation
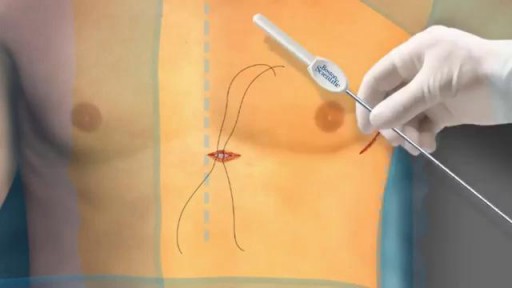
S-ICD leaves the heart and vasculature untouched. It may be implanted using only anatomical landmarks, thereby eliminating the need for fluoroscopy during implant and therefore reducing radiation exposure for both patients and physicians and eliminating the need for lead apron during implant.
Pancake by a Cardiologist

Bacterial abscess of the liver is relatively rare; however, it has been described since the time of Hippocrates (400 BCE), with the first published review by Bright appearing in 1936. In 1938, Ochsner's classic review heralded surgical drainage as the definitive therapy; however, despite the more aggressive approach to treatment, the mortality remained at 60-80%. [1] The development of new radiologic techniques, the improvement in microbiologic identification, and the advancement of drainage techniques, as well as improved supportive care, have reduced mortality to 5-30%; yet, the prevalence of liver abscess has remained relatively unchanged. Untreated, this infection remains uniformly fatal.

Removing a hump from the bridge is one of the most common things people want addressed during their rhinoplasty. Nasal humps can range widely in size. Perhaps you just have a small bump that you'd like refined? Or maybe you have more of a Roman Nose with a more dominating, distracting large hump? No matter if your nose falls on one of these extremes or somewhere in between rhinoplasty surgery can be used to reshape your nose. For anyone considering having a rhinoplasty to reduce a hump on their bridge there are several things to consider before having surgery.

Skin isn't just your body's biggest organ-- it's also the fastest growing.
Nerve damage can start as numbness or tingling and progress to an intense feeling of burning or stabbing. What to know about treatment options:

GIANT EAR WAX REMOVAL By using the elephant ear device.It's very useful video for medical students.Please share it!
Registered Nurse Ken describes what a real "sore throat"

Ultrasound or ultrasonography is a medical imaging technique that uses high frequency sound waves and their echoes. The technique is similar to the echolocation used by bats, whales and dolphins, as well as SONAR used by submarines. In ultrasound, the following events happen: The ultrasound machine transmits high-frequency (1 to 5 megahertz) sound pulses into your body using a probe. The sound waves travel into your body and hit a boundary between tissues (e.g. between fluid and soft tissue, soft tissue and bone). Some of the sound waves get reflected back to the probe, while some travel on further until they reach another boundary and get reflected. The reflected waves are picked up by the probe and relayed to the machine. The machine calculates the distance from the probe to the tissue or organ (boundaries) using the speed of sound in tissue (5,005 ft/s or1,540 m/s) and the time of the each echo's return (usually on the order of millionths of a second). The machine displays the distances and intensities of the echoes on the screen, forming a two dimensional image like the one shown below.
Multiple myeloma is a cancer formed by malignant plasma cells. Normal plasma cells are found in the bone marrow and are an important part of the immune system.

A boxer's fracture is a break through the bones of the hand that form the knuckles. Some doctors use the term "brawler's fracture" rather than "boxer's fracture" because a boxer is not likely to get this injury. The less well-trained brawlers have to learn how to punch without hurting themselves. The metacarpal bones in the hand connect the bones in the finger to the bones in the wrist. There are five metacarpal bones, one to connect each finger to the wrist. All of the metacarpal bones have the same anatomic structure. Each consists of the base, the shaft, the neck, and the head
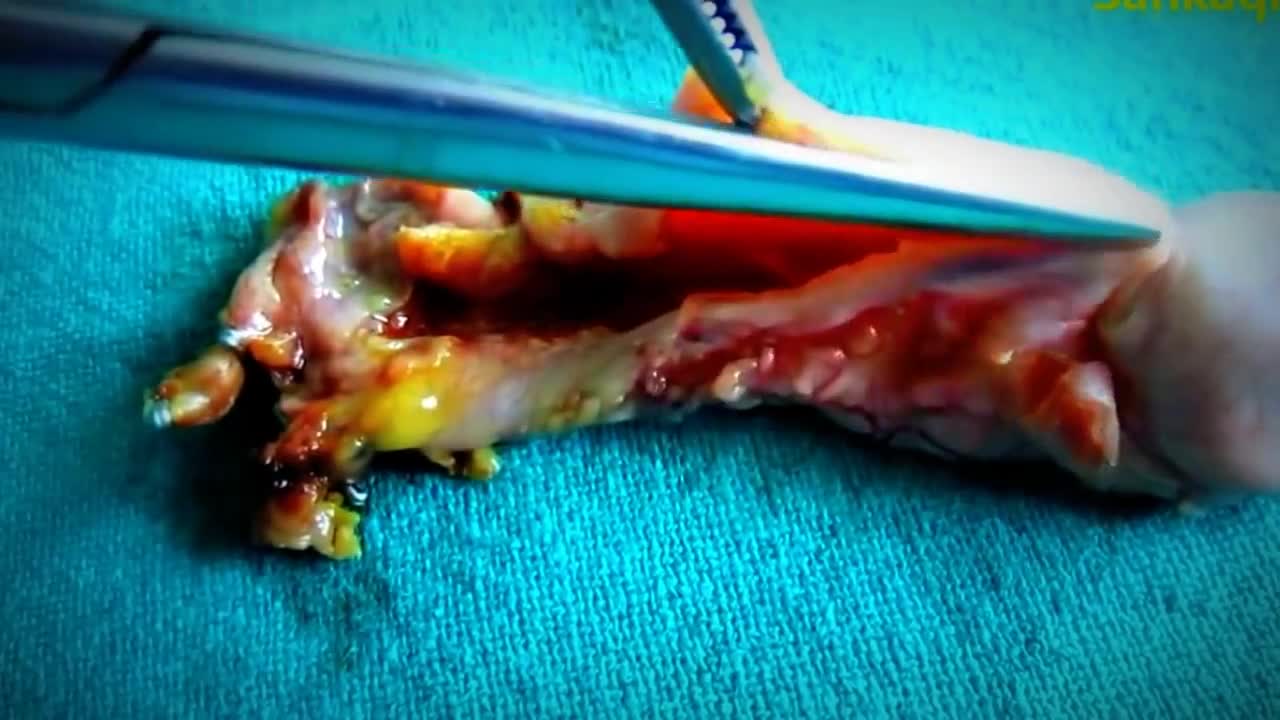
A foot of gauze out of nipple abscess

Art restoration of anterior teeth

http://plantar-fasciitis-solution.info-pro.co Foot Arch Pain, Sharp Pain In Heel, Pain In Foot, Achilles Heel Pain, Chronic Plantar Fasciitis What is Plantar Fasciitis? Plantar fasciitis is a common injury that affects the heel of a person’s foot. The arches of the feet are supported by a tough and fibrous tissue known as the plantar fascia and when this tissue is used repetitively, injury may occur. It can be easy to overuse the feet, especially when participating in activities such as sporting events. Hence, plantar fasciitis is more commonly found in athletes or others who are constantly using their feet for long durations. With excessive use, the planar fascia will eventually give in and this condition may also be progressive. Runners and those who are known to participate in similar activities need to ensure that they do not damage this important band of tissue. In addition, body weight could be a factor that leads to the occurrence of plantar fasciitis. If a person is overweight, the feet and subsequently the plantar fascia tissue could become overwhelmed. Improper footwear could also cause a strain on the plantar fascia tissue and this could gradually become severe over time. plantar fasciitis relief in 7 days click here. http://plantar-fasciitis-solution.info-pro.co
