- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
UCSF Director of Women's Imaging, San Francisco General Hospital, looks at pros and cons of imagining techniques for younger women. Series: "Breast Cancer Prevention and Treatment"

Watch that video to know if it is safe to have intercourse during her period
screening and early detection is the key to beating any form of cancer. share this with a friend. you may save a life.

This animation shows you how a tummy tuck is performed at Boerhaave Medical Centre. Curious? Watch the video!
Boerhaave Medical Centre sets itself the goal of providing the highest quality care. Quality not just in terms of treatment, but also in terms of our staff and the before and after care given. By providing thorough information and clear advice in advance, carefully supporting our patients through the procedure and caring for them afterwards, we believe this quality is assured.
Although we are one of the largest clinics in the Netherlands and have built up many years of experience, we continuously strive to improve. After all, the Boerhaave Medical Centre intends to remain a pioneer in the healthcare sector, by working in accordance with the latest medical findings and techniques both now and in the future.
We offer the highest standard of plastic surgery in our cosmetic care department. For 365 days a year, you can also come to us for non-surgical treatments, such as injectables, permanent hair removal and gastric balloons.
We have been awarded the ZKN quality mark and are certified to ISO 9001-2008 for giving advice and carrying out plastic surgery, including after care.
Visit our website for more information: https://www.boerhaave.com/all-....treatments/upperbody
Follow us:
Facebook: https://www.facebook.com/boerhaavemc
Google+: https://plus.google.com/+BoerhaaveNl-Kliniek
Pinterest: https://nl.pinterest.com/BoerhaaveMC/
Instagram: https://www.instagram.com/BoerhaaveMC/

Watch that Human Baby Medical Abortion Surgery

Laringectomia total ampliada en carcinoma laringeo avanzado T4a. Hospital Dr Sotero del Rio

PREPARING FOR GYNECOMASTIA SURGERY - This maybe the first time you are planning to undergo surgery. It's natural to feel little anxious about the whole process. Get more information www.bestbreastsurgeryindia.com | www.themedspa.us/cosmetic-surgery/male-breast-reduction.html

It’s called gamma knife surgery, but there’s no cutting involved.
It’s been used at Mayo Clinic for 30 years as an alternative to open brain surgery.
The patient’s head is held still during the procedure with a headframe, which also serves as a map for the radiation. Using 3D imaging — typically an MRI — as a guide, the gamma knife is targeted directly at the tumor.
And with no hospital stay and minimal side effects, it’s a procedure that is efficient and can be lifesaving.
More health and medical news on the Mayo Clinic News Network. https://newsnetwork.mayoclinic.org/
Journalists: Clean and nat sound versions of this pkg available for download at https://newsnetwork.mayoclinic.org/
Register (free) at https://newsnetwork.mayoclinic.org/request-account/
Scoliosis is a sideways curvature of the spine that occurs most often during the growth spurt just before puberty. While scoliosis can be caused by conditions such as cerebral palsy and muscular dystrophy, the cause of most scoliosis is unknown.
mply put, relapses, also known as flare ups, or (MS) attacks are new or worsening MS symptoms. But there is a concrete definition used by healthcare providers to identify MS attacks. To be considered an MS relapse: Old symptoms of MS must have become worse or new symptoms appeared.
The 3rd Annual W. B. Ingalls Memorial
Prostate Health and Cancer Seminar features nationally renowned physicians and scientists presenting the most current study and practices for the diagnosis and treatment of prostate cancer. This day-long program offers in-depth exploration of prostate issues that range from monitoring PSA counts to cutting-edge research to current treatment trends.
15th August Special Offer - Get 50% discount on Chemical Peel & Medical Facial ! offer valid till 31st August 2018 ! Call now 09958221983 to book appointment! Send your Query: info@drkashyap.com #MedicalFacial #ChemicalPeels #Facial #SkinCare #NonSurgical #Treatments #Clinic #Delhi #India #15thAugust #IndependenceDay
A diaphragm is a shallow, bendable cup that you put inside your vagina. It covers your cervix during sex to prevent pregnancy.

exam

Chinese Complete Physical Clinical Exam

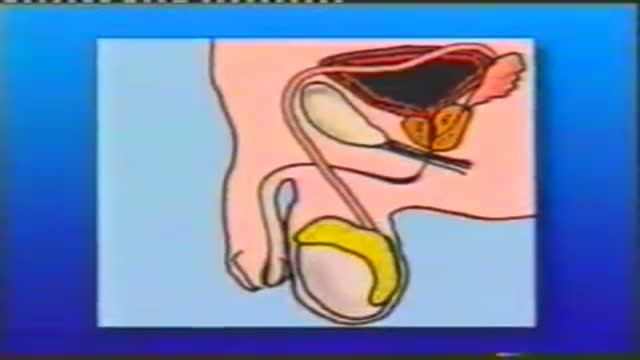
A walk through of an interactive about male to female sex reassignment surgery.

http://control-blood-sugar.good-info.co Low Blood Sugar, Signs Of Low Blood Sugar, Low Iron In Blood, Normal Glucose Levels In Blood Are You Suffering From High Or Uncontrollable Blood Sugar? Because This May Be The Solution. If you’re one of the 387 million people in the world trying to win the battle against uncontrollable blood sugar or even diabetes. Then you’re in the right place, as believe it or not, these conditions can be completely reversed from the comfort of your own home in just 3 short weeks. Are you. Tired of poking your skin with expensive needles everyday? Tired of dealing with the constant lethargy and lack of energy that’s associated with your uncontrollable blood sugar? Tired of living your life with stubborn body fat on your waist, legs,and thighs? Tired of being embarrassed to go to the beach or even taking your shirt off in front of your kids? Tired of waking up with a headache in a soaked bed from sweating so much at night? If you are sick and tired of these all of these conditions and more, then I am happy to tell you that all these conditions of your uncontrollable blood sugar can be completely thrown away for good! click here. http://control-blood-sugar.good-info.co

Watch that video of Dissection Inside Fat Body

Orchidectomy and Orchidopexy in Testicular Torsion

watch that video of Navel stone removal from a dirty bellybutton
