- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Laparoscopic Repair of Rupture Urinary Bladder

Penile Injection Therapy

HPV causes genital warts and cervical and other anogenital cancers. The HPV vaccine is recommended for girls and women 9 to 26 years of age to reduce infections, but information on safety in pregnant women is limited.

Female condoms are easy to use with a little practice. Here are the basics on how to insert, use, and remove a female condom.
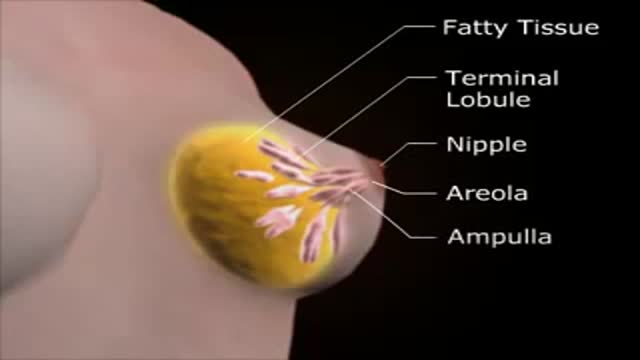
Medical Female Breast Exam
Multiple sclerosis (MS) is a potentially disabling disease of the brain and spinal cord (central nervous system). In MS, the immune system attacks the protective sheath (myelin) that covers nerve fibers and causes communication problems between your brain and the rest of your body. Eventually, the disease can cause the nerves themselves to deteriorate or become permanently damaged. Signs and symptoms of MS vary widely and depend on the amount of nerve damage and which nerves are affected. Some people with severe MS may lose the ability to walk independently or at all, while others may experience long periods of remission without any new symptoms. There's no cure for multiple sclerosis. However, treatments can help speed recovery from attacks, modify the course of the disease and manage symptoms

Dr. Linder is removing a patients breast implants after having five breast augmentations from three previous surgeons. She has baker 4 capsular contracture and is look forward to having them removed. The most common reasons for removing a breast implant include; heath reasons such as back pain, reoccurring complications and the desire for a different shape or size. For implant removal surgery, Dr. Linder makes an inframammary incision (along the breast crease). The implant can be removed intact, or it may need to be punctured before removal. An antibiotic solution is used to irrigate the breast pocket after implant removal. For more information about breast implant removal go to www.implantremoval.net or call Dr. Linder's office at 310-275-4513
The mainstay of treatment is usually medication, talk therapy, or a combination of the two. Increasingly, research suggests these treatments may normalize brain changes associated with depression.

A cervical rib in humans is an extra rib which arises from the seventh cervical vertebra. Sometimes known as "neck ribs", their presence is a congenital abnormality located above the normal first rib. A cervical rib is estimated to occur in 0.2% (1 in 500 people) to 0.5% of the population.

Loyola Full Male Exam Part 2 A video from Loyola medical school, Chicago showing the full examination of the male
Dark Circles around Eyes


In a normal person, when a muscle tendon is tapped briskly, the muscle immediately contracts due to a two-neuron reflex arc involving the spinal or brainstem segment that innervates the muscle. The afferent neuron whose cell body lies in a dorsal root ganglion innervates the muscle or Golgi tendon organ associated with the muscles; the efferent neuron is an alpha motoneuron in the anterior horn of the cord. The cerebral cortex and a number of brainstem nuclei exert influence over the sensory input of the muscle spindles by means of the gamma motoneurons that are located in the anterior horn; these neurons supply a set of muscle fibers that control the length of the muscle spindle itself.

Ingrown Hair Removal Video
A diagnosis of sarcoidosis is established on the basis of compatible clinical and radiologic findings and histologic evidence of the presence of noncaseous epithelioid cell granulomas in one or more organs and the absence of causative organisms or particulates (16). Granulomas of known causes and local sarcoidlike reactions must be excluded. Granulomatous lesions may result from many conditions, including tuberculosis, berylliosis, leprosy, hypersensitivity pneumonitis, Crohn disease, primary biliary cirrhosis, and fungal disease. Moreover, local sarcoidlike reactions may be seen in lymph nodes that drain a neoplasm or a site of chronic inflammation (19). Such reactions also have been seen in patients who have undergone chemotherapy and radiation therapy (23). If biopsy of lymph nodes or pulmonary or pleural tissue is necessary for diagnosis, one of three techniques may be used: transbronchial biopsy, CT-guided biopsy, or surgical biopsy (24). The use of a surgical technique may be warranted when the results of biopsy with another procedure are not definitive and biopsy of mediastinal lymph nodes, lung, or both is required. This can generally be done with minimally invasive procedures, such as cervical mediastinoscopy, the Chamberlain procedure (a parasternal minithoracotomy for biopsy of the aortopulmonary window or para-aortic nodes), or video-assisted thoracoscopic surgical biopsy (25).

A spermatocele (SPUR-muh-toe-seel) is an abnormal sac (cyst) that develops in the epididymis — the small, coiled tube located on the upper testicle that collects and transports sperm. Noncancerous and generally painless, a spermatocele usually is filled with milky or clear fluid that might contain sperm. The exact cause of spermatoceles is unknown but might be due to a blockage in one of the tubes that transports sperm. Spermatoceles, sometimes called spermatic cysts, are common. They typically don't reduce fertility or require treatment. If a spermatocele grows large enough to cause discomfort, your doctor might suggest surgery.

If your knee is severely damaged by arthritis or injury, it may be hard for you to perform simple activities, such as walking or climbing stairs. You may even begin to feel pain while you are sitting or lying down. If nonsurgical treatments like medications and using walking supports are no longer helpful, you may want to consider total knee replacement surgery. Joint replacement surgery is a safe and effective procedure to relieve pain, correct leg deformity, and help you resume normal activities. Knee replacement surgery was first performed in 1968. Since then, improvements in surgical materials and techniques have greatly increased its effectiveness. Total knee replacements are one of the most successful procedures in all of medicine. According to the Agency for Healthcare Research and Quality, more than 600,000 knee replacements are performed each year in the United States. Whether you have just begun exploring treatment options or have already decided to have total knee replacement surgery, this article will help you understand more about this valuable procedure.
Basic well-male examination of the genitals and digital rectal exam.

The examination room should be quiet, warm and well lit. After you have finished interviewing the patient, provide them with a gown (a.k.a. "Johnny") and leave the room (or draw a separating curtain) while they change. Instruct them to remove all of their clothing (except for briefs) and put on the gown so that the opening is in the rear. Occasionally, patient's will end up using them as ponchos, capes or in other creative ways. While this may make for a more attractive ensemble it will also, unfortunately, interfere with your ability to perform an examination! Prior to measuring vital signs, the patient should have had the opportunity to sit for approximately five minutes so that the values are not affected by the exertion required to walk to the exam room. All measurements are made while the patient is seated. Observation: Before diving in, take a minute or so to look at the patient in their entirety, making your observations, if possible, from an out-of-the way perch. Does the patient seem anxious, in pain, upset? What about their dress and hygiene? Remember, the exam begins as soon as you lay eyes on the patient. Temperature: This is generally obtained using an oral thermometer that provides a digital reading when the sensor is placed under the patient's tongue. As most exam rooms do not have thermometers, it is not necessary to repeat this measurement unless, of course, the recorded value seems discordant with the patient's clinical condition (e.g. they feel hot but reportedly have no fever or vice versa). Depending on the bias of a particular institution, temperature is measured in either Celcius or Farenheit, with a fever defined as greater than 38-38.5 C or 101-101.5 F. Rectal temperatures, which most closely reflect internal or core values, are approximately 1 degree F higher than those obtained orally. Respiratory Rate: Respirations are recorded as breaths per minute. They should be counted for at least 30 seconds as the total number of breaths in a 15 second period is rather small and any miscounting can result in rather large errors when multiplied by 4. Try to do this as surreptitiously as possible so that the patient does not consciously alter their rate of breathing. This can be done by observing the rise and fall of the patient's hospital gown while you appear to be taking their pulse. Normal is between 12 and 20. In general, this measurement offers no relevant information for the routine examination. However, particularly in the setting of cardio-pulmonary illness, it can be a very reliable marker of disease activity. Pulse: This can be measured at any place where there is a large artery (e.g. carotid, femoral, or simply by listening over the heart), though for the sake of convenience it is generally done by palpating the radial impulse. You may find it helpful to feel both radial arteries simultaneously, doubling the sensory input and helping to insure the accuracy of your measurements. Place the tips of your index and middle fingers just proximal to the patients wrist on the thumb side, orienting them so that they are both over the length of the vessel.