- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Watch that Female Genital Walls Tightening Plastic Surgery

Watch that Full Real Human Body Decomposition Process

Mouth ulcers are sores that appear in the mouth, often on the inside of the cheeks. Mouth ulcers, also known as aphthous ulcers, can be painful when eating, drinking or brushing teeth. Occasional mouth ulcers are usually harmless and clear up on their own. Seek medical advice if they last longer than 3 weeks or keep coming back. Mouth ulcers cannot be caught from someone else. Up to 1 in 5 people get recurrent mouth ulcers.

: Frederick Lang, M.D., and Jeffrey Weinberg, M.D., neurosurgeons at MD Anderson Cancer Center, answer frequently asked questions about what to expect when you’re having brain tumor surgery.
Learn more about the MD Anderson Brain and Spine Center: www.mdanderson.org/brainandspine
Request an appointment at MD Anderson by calling 1-877-632-6789 or online: https://my.mdanderson.org/RequestAppointment
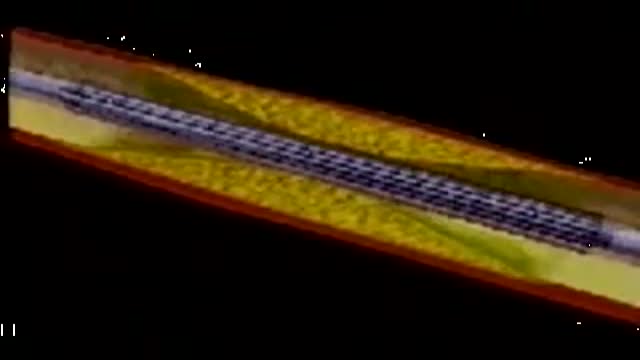
This video depicts how a stent is placed in the coronary artieries. We first place a guiding wire in the heart artery through a catheter, usually from the groin. Then the stent is inflated by a balloon in the artery, which is then removed. The stent remains permanently. Blood thinners, aspirin and plavix, are both required after a stent is placed in your heart artery.

Remove a Plantar Wart from a foot Procedure

Must Watch Very Special New Funny Video 2023 Doctor Funny Video Injection Wala Funny Video | Comedy Video Episode 124 By Fun Comedy Ltd
@funcomedyltd
#funcomedyltd
#doctor
#comedy
#wala
Hello Dear Viewers,
If We have any mistake. please comment and tell us, what is our mistake? We will try to solve this mistake next. please watch our videos and give us confidence to trying best. Thank you for watching this video.
IMPORTANT NOTE:-
This video are no any kind of risk. This video are totally acting no risk no Dangerous act no Physical Harm or Death its ok for viewers.
injection wala comedy video injection wala video injection funny video injection injection wala injection injection doctor doctor doctor sui wala wala suji wala suji wala cartoon doctor cartoon funny video tui tui injection cartoon 22 cartoon video injection video cartoon cartoon comedy video doctor video wala cartoon busy fun ltd my family our fun tv fun tv 24 fun tv 420 funny day funny family ding dong bidik fun tv roma fun tv
#cartoon
#comedyvideo
#doctor_doctor
#busyfunltd
#newfunnyvideo2022
#newfunniestcomedy
#injectionfunnyvideo
#sui_wala
#myfamily
#busyfunltd
#funnyday
#bidikfuntv
#mohafuntv
#dingdong

This video demonstrates how to perform an abdominal examination in an OSCE station.
You can access our step-by-step OSCE guide to accompany this video here: https://geekymedics.com/abdominal-examination/
Check out our other awesome clinical skills resources including:
• 🔥 Geeky Medics Bundles (discounted products): https://app.geekymedics.com/purchase/bundles/
• ✨ 1000+ OSCE Stations: https://app.geekymedics.com/pu....rchase/osce-stations
• 🏥 Geeky Medics OSCE Revision Book: https://app.geekymedics.com/purchase/book/
• 📝 150+ PDF OSCE Checklists: https://geekymedics.com/pdf-osce-checklists/
• 🗂️ 3000+ OSCE Flashcards: https://app.geekymedics.com/pu....rchase/flashcard-col
• 📱 Geeky Medics OSCE App: https://geekymedics.com/geeky-medics-app/
• 🩺 Medical Finals SBA Question Pack: https://app.geekymedics.com/pu....rchase/medical-stude
• 💊 PSA Question Pack: https://app.geekymedics.com/pu....rchase/prescribing-s
Chapters:
- Introduction 00:00
- General inspection 00:35
- Hands 00:47
- Asterixis 01:20
- Arms and axilla 01:32
- Face, eyes & mouth 01:45
- Lymph node palpation 02:19
- Chest inspection 02:50
- Inspection of abdomen 03:02
- Palpation of abdomen 03:34
- Percussion of abdomen 05:36
- Shifting dullness 06:30
- Auscultation of abdomen 06:55
- Summary 07:29
Subscribe to our newsletter to be the first to know about our latest content: https://geekymedics.com/newsletter/ ✉️
Join the Geeky Medics community: 👩👩👧👧
Twitter: http://www.twitter.com/geekymedics
Instagram: https://instagram.com/geekymedics
Facebook: http://www.facebook.com/geekymedics
Always adhere to your medical school/local hospital guidelines when performing examinations or clinical procedures. DO NOT perform any examination or procedure on patients based purely upon the content of these videos. Geeky Medics accepts no liability for loss of any kind incurred as a result of reliance upon the information provided in this video.
Some people have found this video useful for ASMR purposes.
FREE Nursing School Cheat Sheets at: http://www.NURSING.com
Get the full lesson on IM Injections here:
https://nursing.com/lesson/ski....lls-06-01-pill-crush
Check out our new Nurse Care Plan Lessons here:
https://bit.ly/3BPRfPL
Get Access to Thousands of Lessons here:
https://nursing.com/courses/
Welcome to the NURSING Family, we call it the most supportive nursing cohort on the planet.
At NURSING.com, we want to help you remove the stress and overwhelm of nursing school so that you can focus on becoming an amazing nurse.
Check out our freebies and learn more at: (http://www.nursing.com)
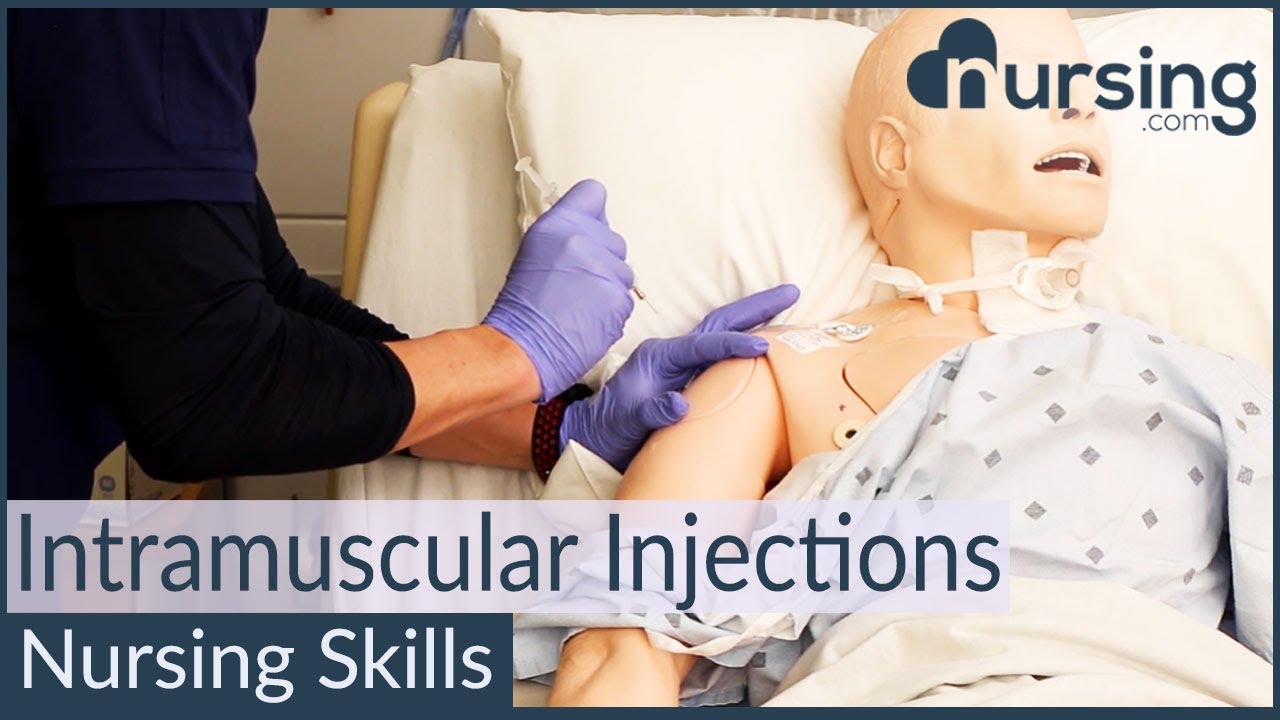
Intramuscular Injection Techniques (Nursing Skills)
In this video, we’re going to look at proper administration techniques for intramuscular medication administration. Of course, always follow your 5 rights and calculate the correct volume for administration. We love you guys! Go out and be your best selves today! And, as always, happy nursing!
Bookmarks:
0.05 Introduction to Intramuscular injections
0.16 site and needle selection
0.35 site sterilization
0.43 Z track method
0.58 needle insertion
1.10 medication injection
1.14 needle removal
1.25 bandaging and needle disposal
1.30 documentation and patient monitoring
1.35 Outro
Visit us at https://nursing.com/medical-disclaimer/ for disclaimer information.
NCLEX®, NCLEX-RN® are registered trademarks of the National Council of State Boards of Nursing, INC. and hold no affiliation with NURSING.com.

Liposuction in tummy tuck requires special planning and technique. I need to ensure that the blood circulation is well maintained for good healing. Yet proper liposuction is important to have a nice flat and contoured tummy.
#hdliposuction #tummytuck #lipoabdominoplasty #surgicalplanning #skinremovalsurgery #imeediatelyafter #plasticsurgeondubai #cocoonaclinic #drsanjayparashar #dubai
For more information visit www.drsanjayparashar.com
For more content, follow me on my social media
Instagram : https://www.instagram.com/drsanjayparashar/
Facebook : https://www.facebook.com/drsanjayparashar

(cryptorchidism) is a testicle that hasn't moved into its proper position in the bag of skin hanging below the penis (scrotum) before birth. Usually just one testicle is affected, but about 10 percent of the time both testicles are undescended. An undescended testicle is uncommon in general, but common among baby boys born prematurely. The vast majority of the time, the undescended testicle moves into the proper position on its own, within the first few months of life. If your son has an undescended testicle that doesn't correct itself, surgery can relocate the testicle into the scrotum.

Vasectomy is a minor surgical procedure wherein the vasa deferentia of a man are severed, and then tied or sealed in a manner such to prevent sperm from entering the seminal stream (ejaculate). Typically done in an outpatient setting, a traditional vasectomy involves numbing (local anesthetic) of the scrotum after which 1 (or 2) small incisions are made, allowing a surgeon to gain access to the vas deferens.

The Epley maneuver or repositioning maneuver is a maneuver used to treat benign paroxysmal positional vertigo of the posterior or anterior canals
| MBBS मतलब JOHARI MBBS I
Download Johari MBBS APP ( For Online LIVE Classes, Notes, Books PDFs, Test Series )
Johari MBBS ( iPhone IOS Users ) LINK { FOR Online LIVE Classes }
https://apps.apple.com/in/app/....johari-mbbs/id647466
JOHARI MBBS APP ( Android ) LINK { FOR Online LIVE Classes }
https://play.google.com/store/....apps/details?id=co.d
CRASH COURSE LINK ( Anatomy in 30Days with Biochemistry In 7Days Series )
https://zczob.on-app.in/app/oc/389813/zczob
IMPORTANT LINKS :-
1) ORDER Anatomy Next Edition Module , Biochemistry in 7Days & Physiology MODULE
https://joharimbbs.com/
2) Join INSTAGRAM ( For Notes, Revision REELs, Updates )
https://www.instagram.com/johari_mbbs_lectures/
3) INSTA Broadcast Channel ( FOR Daily VLOGS, Life Update )
https://ig.me/j/Abal9xRcXcUyrYpT/
4) Telegram ( For FREE BOOKS PDFs )
https://t.me/joharimbbsofficial
5) Whatsapp Channel ( Daily Update )
https://whatsapp.com/channel/0....029VaEeWKWHAdNb0xOzl
6) Follow On Twitter ( For Latest Updates )
https://twitter.com/JohariMbbs
CRASH COURSE LINK ( Anatomy in 30Days with Biochemistry In 7Days Series )
https://zczob.on-app.in/app/oc/389813/zczob
#mbbs #joharimbbs #anaatomy #biochemistry #physiology #medico #doctors
histology slide identification tricks
histology slides identification tricks
histology slide
histology slides
histology slides identification
histology slide preparation
histology slides identification epithelium
histology slides identification connective tissue
histology slides identification tricks
histology slides of epithelium
histology slide identification
#anatomy#clinicalanatomy #MBBS #neroanatomy #bdc #medsudent #medicalcollege
For notes IG - johari_mbbs_lectures
link- https://www.instagram.com/p/CNOwFgEJmJL/
Join Telegram Channel ( JOhari MBBS Public 20x )
https://t.me/JohariMBBS
For Tag :-
histology , histology slides , histology slide identification , histology slides identification , histology slides preparation , tongue histology slide , histology slides asked in exam , histology slide identification trick , histology slides of connective tissue , mbbs histology , histology slides identification epithelium , trachea histology slide , slides , duodenum histology slide , histology slides tricks , histology slides review , examine histology slides

Cardiovascular Examination Clinical skills - Medical School Revision - Dr Gill
The cardiac exam is one of the clinical skills that medical students learn completely, as more often than not, patients will consult regularly about chest pain, and it is important to be able to identify key cardiovascular signs
As a junior doctor, the examination of the cardiovascular system can be almost a dreaded examination, as cardiac murmurs can literally take years of exposure in order to gain confidence with their identification through cardiac auscultation.
This video demonstrates not merely the examination of the heart, but the complete cardiovascular system including its peripheries.
I hope these clinical skill revision videos are helpful, please like and subscribe and join the community so that we can create more effective videos to help with your journey through medical school
#ClinicalExamination #ASMR #drgill
Some people have found this video useful for ASMR
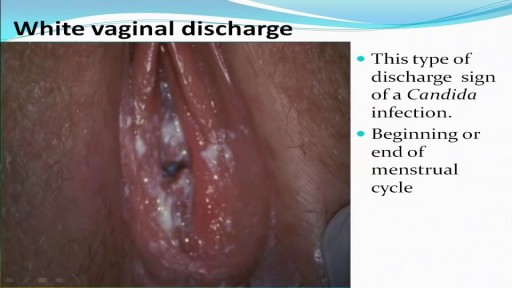
All you need to know about the Types of Female Genital Discharge

Most women have vaginal discharge at many different times throughout their cycle. During ovulation, white and watery discharge is common and accepted as normal. But, discharge after ovulation is widely believed to be a sign of pregnancy.

Watch that video to learn How to Know When You Are Ovulating
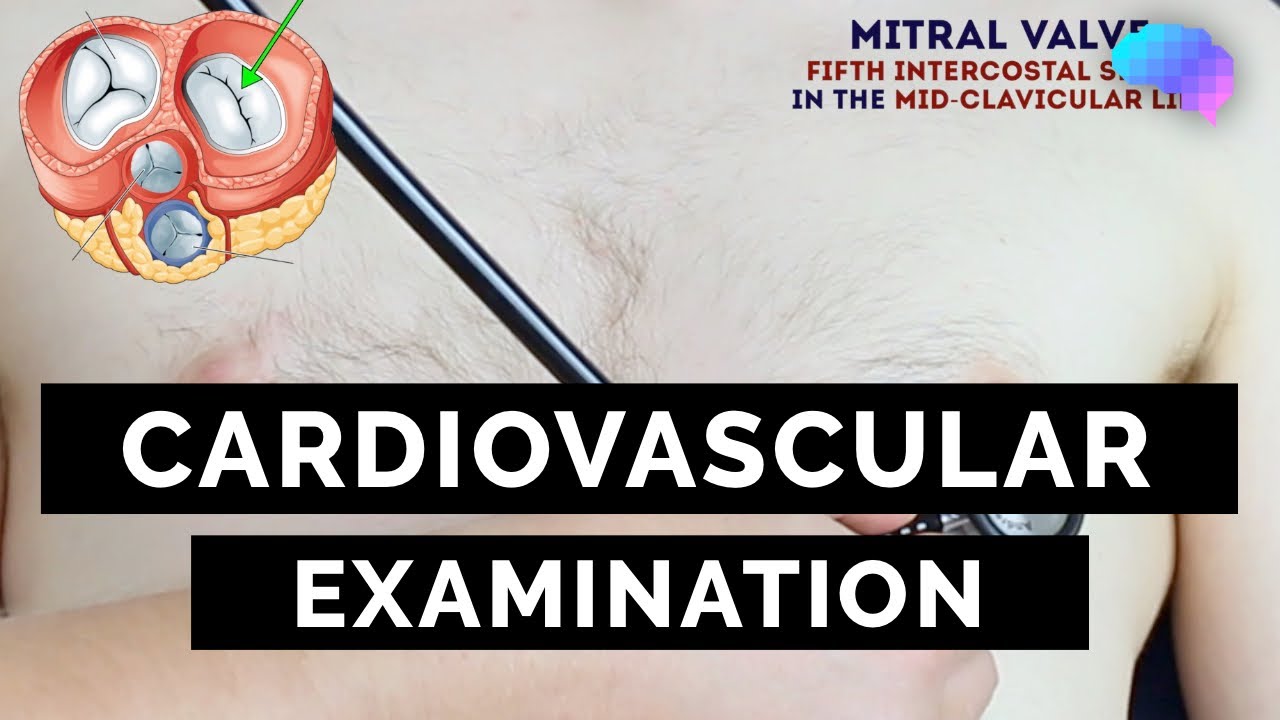
This video demonstrates how to perform a cardiovascular examination in an OSCE station.
You can access our step-by-step OSCE guide to accompany this video here: https://geekymedics.com/cardio....vascular-examination
Check out our other awesome clinical skills resources including:
• 🔥 Geeky Medics Bundles (discounted products): https://app.geekymedics.com/purchase/bundles/
• ✨ 1000+ OSCE Stations: https://app.geekymedics.com/pu....rchase/osce-stations
• 🏥 Geeky Medics OSCE Revision Book: https://app.geekymedics.com/purchase/book/
• 📝 150+ PDF OSCE Checklists: https://geekymedics.com/pdf-osce-checklists/
• 🗂️ 3000+ OSCE Flashcards: https://app.geekymedics.com/pu....rchase/flashcard-col
• 📱 Geeky Medics OSCE App: https://geekymedics.com/geeky-medics-app/
• 🩺 Medical Finals SBA Question Pack: https://app.geekymedics.com/pu....rchase/medical-stude
• 💊 PSA Question Pack: https://app.geekymedics.com/pu....rchase/prescribing-s
Chapters:
- Introduction 00:00
- General inspection 00:35
- Hands 00:46
- Schamroth's window test 01:07
- Capillary refill 01:27
- Pulses 01:35
- Carotid auscultation 02:21
- Carotid pulse 02:43
- Jugular venous pressure 02:55
- Hepatojugular reflux 03:09
- Inspection of the face 03:21
- Inspection of the chest 03:49
- Apex beat 04:12
- Heaves and thrills 04:28
- Heart valve ausculation 04:49
- Accentuation manoeuvres 05:45
- Lung base auscultation 06:23
- Sacral and pedal oedema 06:43
- Summary 07:10
Subscribe to our newsletter to be the first to know about our latest content: https://geekymedics.com/newsletter/ ✉️
Join the Geeky Medics community: 👩👩👧👧
Twitter: http://www.twitter.com/geekymedics
Instagram: https://instagram.com/geekymedics
Facebook: http://www.facebook.com/geekymedics
Always adhere to your medical school/local hospital guidelines when performing examinations or clinical procedures. DO NOT perform any examination or procedure on patients based purely upon the content of these videos. Geeky Medics accepts no liability for loss of any kind incurred as a result of reliance upon the information provided in this video.
Normal heart sounds and aortic regurgitation/stenosis sounds
Recorded on a Thinklabs Digital Stethoscope (https://www.thinklabs.com)
Some people have found this video useful for ASMR purposes.
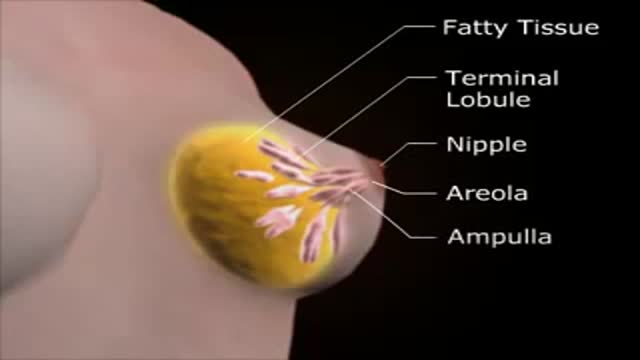
Medical Female Breast Exam
