- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Watch that video of an Ingrown Hair Causes Huge Tumor in a Man's Stomach

Stephen Slade shows a 1 week post op patient after DSAEK. DSAEK is an excellent option for many patients with corneal disease. In DSAEK, only the thin, inner layer is replaced, so the healing is typically much faster than a full thickness cornea graft.

Hip dysplasia is the medical term for a hip socket that doesn't fully cover the ball portion of the upper thighbone. This allows the hip joint to become partially or completely dislocated

The goal of breast cancer surgery is to remove the entire tumor from the breast. Some of the lymph nodes in the underarm area (axillary nodes) may also be removed to see if cancer cells are present.
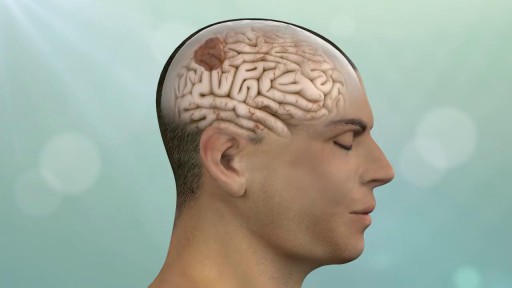
Keyhole surgery can be helpful for patients with brain, pituitary and skull base tumors. With cutting edge technology and a proven track record in keyhole and endonasal endoscopic approaches, we make surgery safer, less invasive and more effective.

How Did Insects Evolve To Feast On Your Blood?

Unstable ankle joints after internal fixation of type B malleolar fractures exist. Residual instability most often occurs after trimalleolar fractures with initial joint dislocation. Treatment with an additional positioning screw generally produced a satisfactory result.


Robotic Surgery Demonstration Using Da Vinci Surgical System
this animated surgery showing management of bone defects with the Precice Lengthening-Compression IM nail


This film explains how dialysis works. It features patients talking about different types of dialysis and how they fit the treatment into their lives.

A growing number of patients having total knee replacement surgery are 55 or younger. Surgeons at Sunnybrook's Holland Centre perform more than 1,000 total knee replacements each year. Read more: http://sunnyview.sunnybrook.ca..../2011/11/snap-crackl

Peripheral vascular disease, also called PVD, refers to any disease or disorder of the circulatory system outside of the brain and heart. The term can include any disorder that affects any blood vessels. It is, though, often used as a synonym for peripheral artery disease. PVD is the most common disease of the arteries. The build-up of fatty material inside the vessels, a condition called atherosclerosis or hardening of the arteries, is what causes it. The build up is a gradual process. Over time, the artery becomes blocked, narrowed, or weakened.

A video from Harvard medical school showing Paracentesis

This video shows a surgeon's view during vitrectomy for macular pucker and indocyanine green assisted removal of the ILM.

Inspection of the mouth

How to perform a lumbar puncture.

Surgical removal of a Chalazion from the eye lid

عملية تجميل أو اعادة شكل الانف
د. محمد الروبى
استشارى جراحات التجميل - جامعة عين شمس
