- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Why is this medication prescribed? Amiodarone is used to treat and prevent certain types of serious, life-threatening ventricular arrhythmias (a certain type of abnormal heart rhythm when other medications did not help or could not be tolerated. Amiodarone is in a class of medications called antiarrhythmics. It works by relaxing overactive heart muscles. How should this medicine be used? Amiodarone comes as a tablet to take by mouth. It is usually taken once or twice a day. You may take amiodarone either with or without food, but be sure to take it the same way each time.Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take amiodarone exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
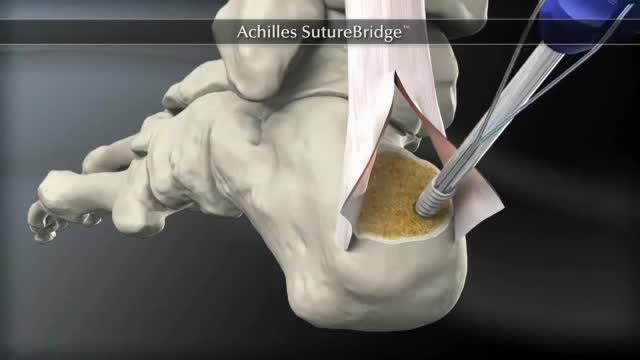
The Arthrex SpeedBridge™ is an innovative soft tissue fixation device used in the treatment of Achilles injuries. While standard anchor fixation of the tendon creates only a single point of compression directly over the anchor, the SpeedBridge enables an hourglass pattern of FiberTape® suture to be laid over the distal end of the tendon. This four-anchor construct enables a true knotless repair and a greater area of compression for the Achilles tendon on the calcaneus, improving stability and possibly allowing for earlier return to normal activities.
Different Types of Breasts
Your headache symptoms can help your doctor determine its cause and the appropriate treatment. Most headaches aren't the result of a serious illness, but some may result from a life-threatening condition requiring emergency care. Headaches are generally classified by cause: Primary headaches A primary headache is caused by overactivity of or problems with pain-sensitive structures in your head. A primary headache isn't a symptom of an underlying disease. Chemical activity in your brain, the nerves or blood vessels surrounding your skull, or the muscles of your head and neck (or some combination of these factors) can play a role in primary headaches. Some people may also carry genes that make them more likely to develop such headaches. The most common primary headaches are: Cluster headache Migraine (with and without aura) Tension headache (also known as tension-type headache) Trigeminal autonomic cephalalgia (TAC), such as cluster headache and paroxysmal hemicrania A few headache patterns also are generally considered types of primary headache, but are less common. These headaches have distinct features, such as an unusual duration or pain associated with a certain activity. Although generally considered primary, each could be a symptom of an underlying disease. They include: Chronic daily headaches (for example, chronic migraine, chronic tension-type headache, or hemicranias continua) Cough headaches Exercise headaches Sex headaches Some primary headaches can be triggered by lifestyle factors, including: Alcohol, particularly red wine Certain foods, such as processed meats that contain nitrates Changes in sleep or lack of sleep Poor posture Skipped meals Stress Secondary headaches A secondary headache is a symptom of a disease that can activate the pain-sensitive nerves of the head. Any number of conditions — varying greatly in severity — may cause secondary headaches. Possible causes of secondary headaches include: Acute sinusitis Arterial tears (carotid or vertebral dissections) Blood clot (venous thrombosis) within the brain — separate from stroke Brain aneurysm (a bulge in an artery in your brain) Brain AVM (brain arteriovenous malformation) — an abnormal formation of brain blood vessels Brain tumor Carbon monoxide poisoning Chiari malformation (structural problem at the base of your skull) Concussion Dehydration Dental problems Ear infection (middle ear) Encephalitis (brain inflammation) Giant cell arteritis (inflammation of the lining of the arteries) Glaucoma (acute angle closure glaucoma) Hangovers

Finding a donor heart can be difficult. The heart must be donated by someone who is brain-dead but is still on life support. The donor heart must be matched as closely as possible to your tissue type to reduce the chance that your body will reject it. You are put into a deep sleep with general anesthesia, and a cut is made through the breastbone. Your blood flows through a heart-lung bypass machine while the surgeon works on your heart. This machine does the work of your heart and lungs while they are stopped, and supplies your body with blood and oxygen. Your diseased heart is removed and the donor heart is stitched in place. The heart-lung machine is then disconnected. Blood flows through the transplanted heart, which takes over supplying your body with blood and oxygen. Tubes are inserted to drain air, fluid, and blood out of the chest for several days, and to allow the lungs to fully re-expand.
Tighten Sagging Breasts

Factitious disorder is the term used to describe a pattern of behavior centered on the exaggeration or outright falsifications of one’s own health problems or the health problems of others. Some people with this disorder fake or exaggerate physical problems; others fake or exaggerate psychological problems or a combination of physical and psychological problems. Factitious disorder differs from a pattern of falsified or exaggerated behavior called malingering. While malingerers make their claims out of a motivation for personal gain, people with factitious disorder have no such motivation.
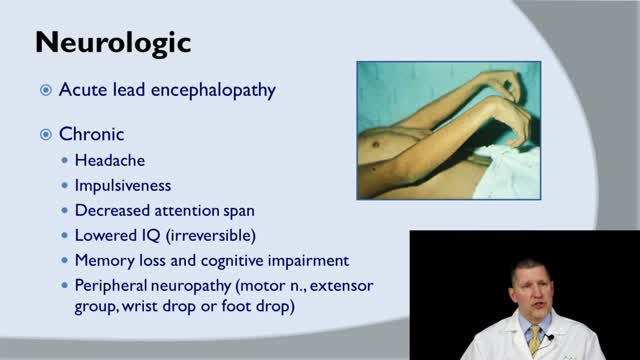
Lead poisoning occurs when lead builds up in the body, often over a period of months or years. Even small amounts of lead can cause serious health problems. Children under the age of 6 are especially vulnerable to lead poisoning, which can severely affect mental and physical development. At very high levels, lead poisoning can be fatal. Lead-based paint and lead-contaminated dust in older buildings are the most common sources of lead poisoning in children. Other sources include contaminated air, water and soil. Adults who work with batteries, do home renovations or work in auto repair shops also may be exposed to lead. While treatment is available for lead poisoning, taking some simple precautions can help protect yourself and your family.
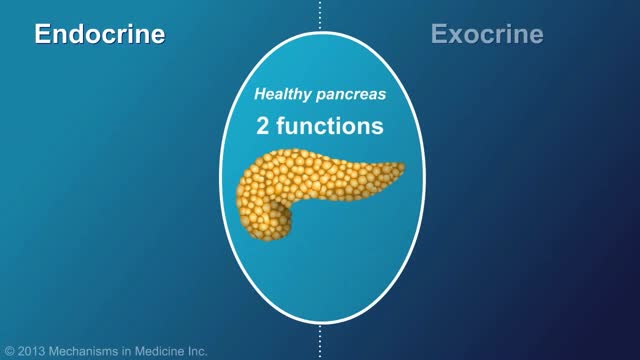
Chronic pancreatitis is a long-standing inflammation of the pancreas that alters the organ's normal structure and functions. It can present as episodes of acute inflammation in a previously injured pancreas, or as chronic damage with persistent pain or malabsorption.
This video: Polycythemia vera (pol-e-sigh-THEE-me-uh VEER-uh) is a slow-growing type of blood cancer in which your bone marrow makes too many red blood cells. Polycythemia vera may also result in production of too many of the other types of blood cells — white blood cells and platelets. These excess cells thicken your blood and cause complications, such as such as a risk of blood clots or bleeding. Polycythemia vera isn't common. It usually develops slowly, and you may have it for years without noticing signs or symptoms. Often, polycythemia vera is found during a blood test done for some other reason. Without treatment, polycythemia vera can be life-threatening. However, with proper medical care, many people experience few problems related to this disease. Over time, there's a risk of progressing to more-serious blood cancers, such as myelofibrosis or acute leukemia.

Claudication is pain caused by too little blood flow, usually during exercise. Sometimes called intermittent claudication, this condition generally affects the blood vessels in the legs, but claudication can affect the arms, too. At first, you'll probably notice the pain only when you're exercising, but as claudication worsens, the pain may affect you even when you're at rest. Although it's sometimes considered a disease, claudication is technically a symptom of a disease. Most often, claudication is a symptom of peripheral artery disease, a potentially serious but treatable circulation problem in which the vessels that supply blood flow to your legs or arms are narrowed. Fortunately, with treatment, you may be able to maintain an active lifestyle without pain.
Influenza is a viral infection that attacks your respiratory system — your nose, throat and lungs. Influenza, commonly called the flu, is not the same as stomach "flu" viruses that cause diarrhea and vomiting. For most people, influenza resolves on its own. But sometimes, influenza and its complications can be deadly. People at higher risk of developing flu complications include: Young children under 5, and especially those under 2 years Adults older than 65 Residents of nursing homes and other long-term care facilities Pregnant women and women up to two weeks postpartum People with weakened immune systems People who have chronic illnesses, such as asthma, heart disease, kidney disease and diabetes People who are very obese, with a body mass index (BMI) of 40 or higher Your best defense against influenza is to receive an annual vaccination.

Indications for intervention in patients with a renal artery aneurysm (RAA) include the following [20, 8, 13, 14] : Rupture Symptomatic RAA - Hypertension (from associated renal artery stenosis, refractory to medical management), pain, renal ischemia or infarction secondary to embolization from the aneurysm sac RAAs in females who are pregnant or are contemplating pregnancy Diameter greater than 2 cm Enlarging RAA RAA associated with acute dissection Currently, there is no consensus regarding the size at which an RAA should be repaired in an asymptomatic patient. Experts have recommended RAA repair at diameters ranging from 1.5 to 3 cm, [8] though most suggest 2 cm. Some reports have even suggest that larger asymptomatic saccular aneurysms may be managed expectantly. Note that aneurysm rupture at a diameter of 1.5 cm has been reported. Complete calcification of the wall of the aneurysm sac manifests in about 40% of patients. This was once believed to confer protection against rupture [21] ; however, this belief has since been questioned. [30] Asymptomatic, small (<2 cm in diameter) RAAs do not usually require treatment. One notable exception is an RAA in a woman who is pregnant or contemplating pregnancy. In view of the increased risk of rupture in such cases, even small asymptomatic aneurysms should be repaired in this population. For diagnosis and preinterventional planning, gadolinium-enhanced magnetic resonance angiography (MRA) and computed tomography (CT) angiography (CTA) with three-dimensional (3D) reconstruction have essentially replaced conventional arteriography. Regular follow-up examination with ultrasonography (US) or CT) is recommended in patients who are treated expectantly. Spontaneous cure by thrombosis of small aneurysms has been described. Further refinements in endovascular techniques may allow more RAAs to be treated in this manner. So far, excellent short- and intermediate-term results have been described in the literature [40] ; however, there remains a need for further long-term outcome data.

Claudication, which is defined as reproducible ischemic muscle pain, is one of the most common manifestations of peripheral arterial occlusive disease (PAOD) caused by atherosclerosis. Claudication occurs during physical activity and is relieved after a short rest. Pain develops because of inadequate blood flow.
Repair of post-infarction ventricular septal defect (VSD) remains a challenging procedure with a high risk of VSD recurrence. In order to reduce this risk, a double patch and glue technique was introduced in the department in 1986. This surgical technique is hereunder presented. Since 1971, ninety-three patients have been operated on early (≪15 days) after the occurrence of a post-infarction VSD. This retrospective study allows to compare the results of this double patch and glue technique to those obtained with the conventional one, in terms of hospital death and VSD recurrence. The double patch and glue technique avoids recurrence of VSD and plays a part in reducing hospital mortality.
Pancreatic Auto Islet Transplantation is a procedure used to maintain insulin production and secretion in patients with chronic pancreatitis that are undergoing a total pancreatectomy, or removal of the entire pancreas. When all other medical therapies fail to control the pain, removal of the pancreas may be an option; however it can leave a person diabetic, which means that the body can no longer control blood sugar levels, and will require intensive testing of blood sugar and injections of insulin. The pancreas is an organ, located in the upper abdominal cavity, behind the stomach, liver and colon. Within the pancreas, specialized clusters of cells known as islets produce insulin, which maintain healthy blood sugar levels. The pancreas also produces enzymes to help digest food. In order to alleviate pain and maintain insulin production, the pancreas is removed from the body, processed and the islets are harvested. Once the pancreas is removed, it is placed in a solution and put into a machine where the pancreas is digested. The islets are then infused into the patient’s liver. Within a short time, the islets are expected to start producing insulin. In 80% of patients, the pain from pancreatitis is relieved by a total pancreatectomy. Over time, some patients may be diabetic and will need to take insulin to maintain healthy blood sugar levels. All patients will take pancreatic enzymes to help digest food after surgery.
An intra-aortic balloon pump (IABP) is a mechanical device that helps the heart pump blood. This device is inserted into the aorta, the body's largest artery. It is a long, thin tube called a catheter with a balloon on the end of it. If you are hospitalized, your doctor may insert an IABP.
Pruritis is itchy skin that makes you want to scratch. It can be caused by many things. Normally, itchy skin isn't serious, but it can make you uncomfortable. Sometimes, itchy skin is caused by a serious medical condition. It can occur in association with a primary rash (e.g. dermatitis) or may occur because of hypersensitive nerves in the skin (neuropathic pruritus). ... Scratching a localised itch may lead to lichen simplex, prurigo or prurigo nodularis. Systemic causes of pruritus. Sytemic diseases may cause generalised pruritus.

If you are self-conscious because you have missing teeth, wear dentures that are uncomfortable or don't want to have good tooth structure removed to make a bridge, talk to your dentist to see if dental implants are an option for you. Dental implants are a popular and effective way to replace missing teeth and are designed to blend in with your other teeth. They are an excellent long-term option for restoring your smile. In fact, the development and use of implants is one of the biggest advances in dentistry in the past 40 years. Dental implants are made up of titanium and other materials that are compatible with the human body. They are posts that are surgically placed in the upper or lower jaw, where they function as a sturdy anchor for replacement teeth.

Most people have general anesthesia right before surgery. This means you will be asleep and pain-free. Other kinds of anesthesia, like regional anesthesia or a block, may also be used for this surgery. The tissue to replace your damaged ACL will come from your own body or from a donor. A donor is a person who has died and chose to give all or part of his or her body to help others. Tissue taken from your own body is called an autograft. The two most common places to take tissue from are the knee cap tendon or the hamstring tendon. Your hamstring is the muscle behind your knee. Tissue taken from a donor is called an allograft. The procedure is usually performed with the help of knee arthroscopy. With arthroscopy, a tiny camera is inserted into the knee through a small surgical cut. The camera is connected to a video monitor in the operating room. Your surgeon will use the camera to check the ligaments and other tissues of your knee. Your surgeon will make other small cuts around your knee and insert other medical instruments. Your surgeon will fix any other damage found, and then will replace your ACL by following these steps: The torn ligament will be removed with a shaver or other instruments. If your own tissue is being used to make your new ACL, your surgeon will make a larger cut. Then, the autograft will be removed through this cut. Your surgeon will make tunnels in your bone to bring the new tissue through. This new tissue will be in the same place as your old ACL. Your surgeon will attach the new ligament to the bone with screws or other devices to hold it in place. As it heals, the bone tunnels fill in. This holds the new ligament in place. At the end of the surgery, your surgeon will close your cuts with sutures (stitches) and cover the area with a dressing. You may be able to view pictures after the procedure of what the doctor saw and what was done during the surgery.
