- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
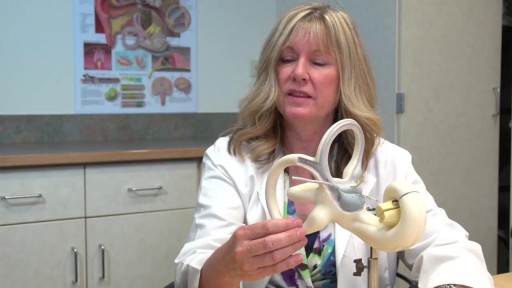
Vertigo is a sensation of feeling off balance. If you have these dizzy spells, you might feel like you are spinning or that the world around you is spinning.

Cervicitis is an inflammation of the cervix, the lower, narrow end of the uterus that opens into the vagina. Possible symptoms of cervicitis include bleeding between menstrual periods, pain with intercourse or during a cervical exam, and abnormal vaginal discharge. However, it's also possible to have cervicitis and not experience any signs or symptoms. Often, cervicitis results from a sexually transmitted infection, such as chlamydia or gonorrhea. Cervicitis can develop from noninfectious causes, too. Successful treatment of cervicitis involves treating the underlying cause of the inflammation.


Otitis media with effusion is inflammation and fluid buildup (effusion) in the middle ear without bacterial or viral infection. This may occur because the fluid buildup persists after an ear infection has resolved. It may also occur because of some dysfunction or noninfectious blockage of the eustachian tubes

مرکز ایمپلنت و زیبایی دندان شیراز دکتر محمد امین دین پرور

Effect of smoking,it's very dangerousAfter watch this video I hope smoker stop smoke now it is dangerously for human

For more information please visit: https://www.yalemedicine.org/c....onditions/acl-injury
Serious injuries, by and large, cause a lot of swelling in the knee. Especially in younger patients. Now, someone could be arthritic and they overdo it going for a big long hike and they get some swelling the next day. But rapid onset of swelling, it's like hard to make out where your kneecap is, is a pretty big cardinal sign that there's something serious that's happened to your knee. Rapid onset swelling is usually due to blood in the joint. "A meniscus that really tears and flips in the front. You tear your quad or your patellar tendon, your kneecap dislocates, you tear a little blood vessel, your ACL tears, a piece of cartilage in bone gets knocked off and causes bleeding. So a lot of the really significant injuries, people get rapid onset swelling within three to four hours and they should seek attention There's always exceptions to rules, but if your knee looks like a grapefruit, you should go get it checked.

Orthopedic surgeon Donald Polakoff, MD describes recovery time from knee replacement surgery.
SUBSCRIBE FOR MORE VIDEOS AND NEWS!
http://www.youtube.com/subscri....ption_center?add_use
CONNECT WITH US!
Google+ ► http://gplus.to/spuh
Facebook ► http://www.fb.com/SaintPetersUniversityHospital
Twitter ► http://twitter.com/sphcs_news
Pinterest ► http://www.pinterest.com/sphcs
Saint Peter's Healthcare System ► http://www.saintpetershcs.com

Mohs surgery is a procedure used to remove skin cancers (most commonly basal and squamous cell carcinoma and melanoma) in a way that preserves a maximum amount of healthy tissue. It is useful for skin cancers when:
(1) the location of the cancer is near sensitive areas, like the fingers or face;
(2) earlier treatments have not worked;
(3) a skin cancer is large; and
(4) regular surgery is less likely to remove the cancer.
This procedure video illustrates the procedure on 2 patients with basal cell carcinoma. Click https://ja.ma/3b4scuY to learn more.
0:00 Disclaimer
0:07 Introduction
0:28 What this video will cover
0:43 Mohs "stage" steps
1:09 Marking surgical sites
1:27 Stage 1: skin layer resection (patient 1)
1:59 Maintaining skin layer orientation
2:55 Stage 1: processing layer onto slides (patient 1)
3:53 Stage 1: histology review for cancer (patient 1)
4:31 Discussion on wound closure
5:10 Wound closure (patient 1)
5:47 Stage 1: histology review for cancer (patient 2)
6:24 Stage 2: skin layer resection (patient 2)
6:38 Stage 2: histology review for cancer (patient 2)
6:56 Stage 3: skin layer resection (patient 2)
7:07 Stage 3: histology review for cancer (patient 2)
7:20 Wound closure (patient 2)
7:57 1-week follow-up before-and-after wound healing

Mr Brian MacCormack talking about Paediatric Surgery Emergencies. This talk is part of the Paediatric Emergencies 2022 event. To get your CME certificate for watching the video please visit https://www.paediatricemergenc....ies.com/conference/p
#PaediatricEmergencies #PaediatricEmergencies2022 #PaediatricSurgery

This request usually follows orbit examination of a patient with thyroid eye disease. The aim is to look for signs of hyperthyroidism and less commonly hypothyroidism.

he appendix is a long narrow tube (a few inches in length) that attaches to the first part of the colon. It is usually located in the lower right quadrant of the abdominal cavity. The appendix produces a bacteria destroying protein called immunoglobulins, which help fight infection in the body. Its function, however, is not essential. People who have had appendectomies do not have an increased risk toward infection. Other organs in the body take over this function once the appendix has been removed.

Examination of the eye,vision,retina and field of vision

Hip examination by Harvard medical school

Removal of a foreign body from the eye (fish hook)

An U/S showing first trimesteric scan

Very Hard White Cataract with trypan blue "Vision blue" Capsule Staining

This patented device replaces cumbersome metal retractors for a variety of surgical procedures. The surgeon has maximum unobstructed exposure and the size of the required incision is minimized.
