- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
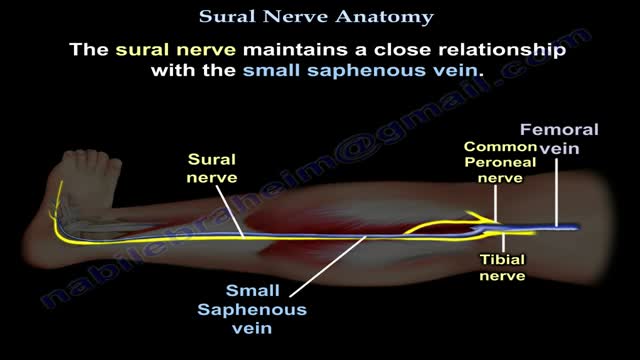
Nerves are the organs that make up the peripheral nervous system (PNS). They serve as information pipelines that allow the brain and spinal cord to communicate with other tissues and organs. Inside the nerves are the axon processes of sensory and motor neurons (nerve cells).

Placenta accreta is the most common accounting for approximately 75% of all cases. Placenta Increta occurs when the placenta attaches even deeper into the uterine wall and does penetrate into the uterine muscle.
First Head Transplant Surgery
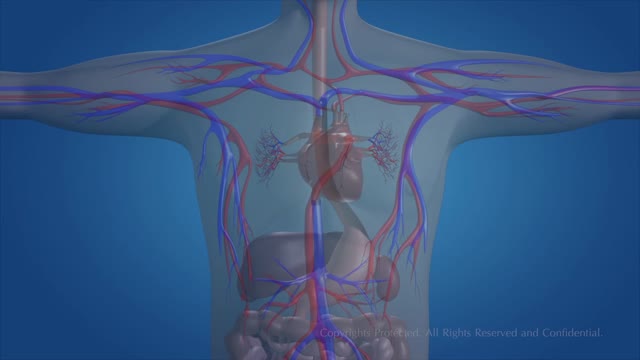
The essential components of the human cardiovascular system are the heart, blood and blood vessels. It includes the pulmonary circulation, a "loop" through the lungs where blood is oxygenated; and the systemic circulation, a "loop" through the rest of the body to provide oxygenated blood.
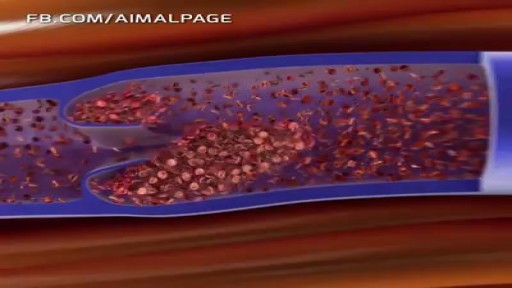
In Deep Vein Thrombosis, blood clot is able to reach the heart and from there it transport to the arteries of the lungs, where it may stuck in the...

Top 10 Foods that Can Kill You
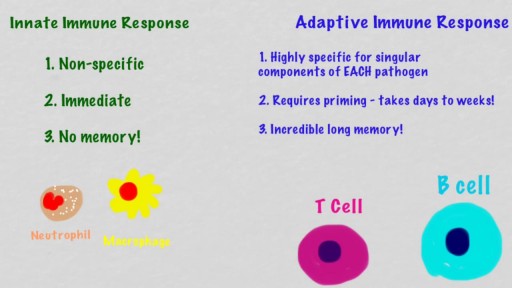
Breast lumps facts Breast lumps can be caused by infections, injuries, non-cancerous growths, and cancer. Breast cancer usually causes no pain in the breast. The symptoms of breast cancer include painless breast lumps, nipple discharge, and inflammation of the skin of the breast. The chances that a particular breast lump could be cancerous depends on many factors, including past medical history, physical examination, as well as genetic and other risk factors. The only way to be certain that a lump is not cancerous is to have a tissue sampling (biopsy). There are several ways to do the biopsy. The treatment of a breast lump depends on its cause.
The cell membrane is selectively permeable to ions and organic molecules and controls the movement of substances in and out of cells. The basic function of the cell membrane is to protect the cell from its surroundings. It consists of the phospholipid bilayer with embedded proteins.
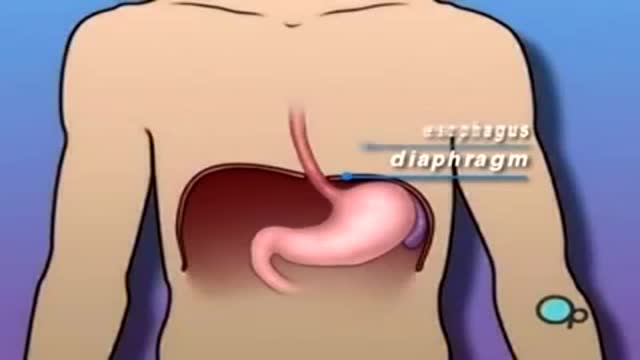
A hiatus hernia or hiatal hernia is the protrusion (or herniation) of the upper part of the stomach into the thorax through the esophageal hiatus because of a tear or weakness in the diaphragm. Hiatus hernias often result in heartburn but may also cause chest pain or pain with eating. The most common cause is obesity.
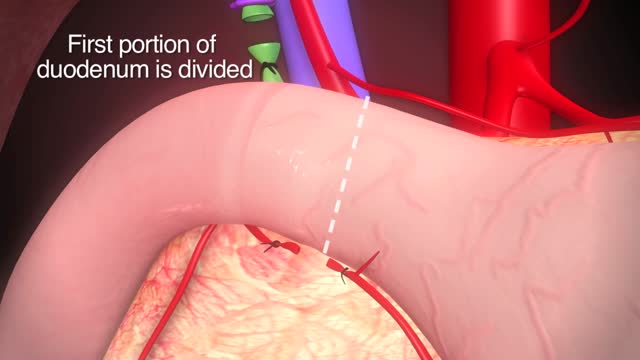
Our specialists treat conditions that are recurrent and hard to treat. Simply put, TPIAT a procedure that lets surgeons remove the pancreas, take out islet cells – the cells in the pancreas that make insulin – and put those islet cells into the liver. Patients then take pancreatic enzymes to help them digest food.

Three cholinesterase inhibitors are commonly prescribed: Donepezil (Aricept) is approved to treat all stages of Alzheimer's. Rivastigmine (Exelon) is approved to treat mild to moderate Alzheimer's. Galantamine (Razadyne) is approved to treat mild to moderate Alzheimer's. Currently, there is no cure for Alzheimer's. But drug and non-drug treatments may help with both cognitive and behavioral symptoms. Researchers are looking for new treatments to alter the course of the disease and improve the quality of life for people with dementia. ... Medications for Memory Loss.
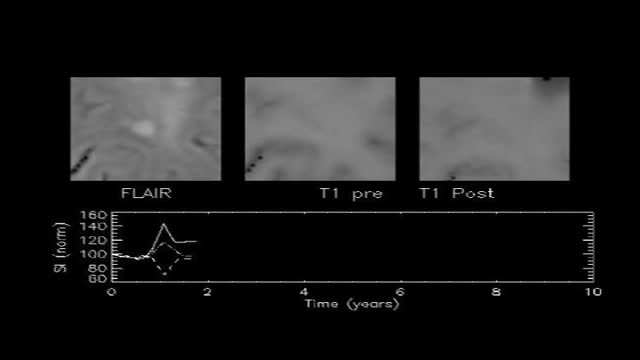
If you have multiple sclerosis (MS), you probably had several tests done before you received your diagnosis. There isn’t one test to diagnosis MS, so testing can vary. Doctors can use neurological exams, information about previous symptoms, blood tests, and spinal fluid tests. A magnetic resonance imaging (MRI) scan isn’t used to diagnose MS but rather to rule out other diseases. A diagnosis of MS requires more information than what a scan alone can give. By looking at more than one test or exam result, doctors can get a clearer picture of what’s going on in your body.
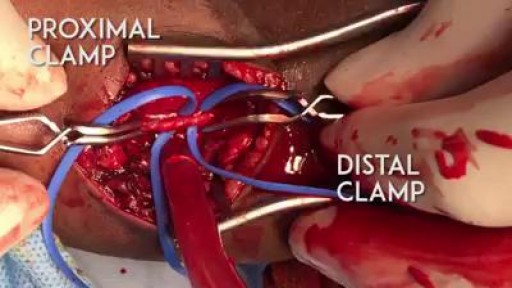
A proper embolectomy should have a good proximal and distal flow to the arteriotomy :)

Lungs Inflating

Baby born without brain

an incision made on the back of the lower leg starting just above the heel bone. After the surgeon finds the two ends of the ruptured tendon, these ends are sewn together with sutures. The incision is then closed. Another repair method makes a small incision on the back of the lower leg at the site of the rupture.
Initially, lead poisoning can be hard to detect — even people who seem healthy can have high blood levels of lead. Signs and symptoms usually don't appear until dangerous amounts have accumulated. Lead poisoning symptoms in children Signs and symptoms of lead poisoning in children include: Developmental delay Learning difficulties Irritability Loss of appetite Weight loss Sluggishness and fatigue Abdominal pain Vomiting Constipation Hearing loss Seizures Eating things, such as paint chips, that aren't food (pica) Lead poisoning symptoms in newborns Babies exposed to lead before birth might: Be born prematurely Have lower birth weight Have slowed growth Lead poisoning symptoms in adults Although children are primarily at risk, lead poisoning is also dangerous for adults. Signs and symptoms in adults might include: High blood pressure Joint and muscle pain Difficulties with memory or concentration Headache Abdominal pain Mood disorders Reduced sperm count and abnormal sperm Miscarriage, stillbirth or premature birth in pregnant women Causes Lead is a metal that occurs naturally in the earth's crust, but human activity — mining, burning fossil fuels and manufacturing — has caused it to become more widespread. Lead was also once used in paint and gasoline and is still used in batteries, solder, pipes, pottery, roofing materials and some cosmetics. Lead in paint Lead-based paints for homes, children's toys and household furniture have been banned in the United States since 1978. But lead-based paint is still on walls and woodwork in many older homes and apartments. Most lead poisoning in children results from eating chips of deteriorating lead-based paint. Water pipes and imported canned goods Lead pipes, brass plumbing fixtures and copper pipes soldered with lead can release lead particles into tap water. Lead solder in food cans, banned in the United States, is still used in some countries. Other sources of lead exposure Lead sometimes can also be found in: Soil. Lead particles from leaded gasoline or paint settle on soil and can last years. Lead-contaminated soil is still a major problem around highways and in some urban settings. Some soil close to walls of older houses contains lead. Household dust. Household dust can contain lead from lead paint chips or from contaminated soil brought in from outside. Pottery. Glazes found on some ceramics, china and porcelain can contain lead that can leach into food served or stored in the pottery. Toys. Lead is sometimes found in toys and other products produced abroad. Cosmetics. Tiro, an eye cosmetic from Nigeria, has been linked to lead poisoning. Herbal or folk remedies. Lead poisoning has been linked to greta and azarcon, traditional Hispanic medicines, as well as some from India, China and other countries. Mexican candy. Tamarind, an ingredient used in some candies made in Mexico, might contain lead. Lead bullets. Time spent at firing ranges can lead to exposure. Occupations. People are exposed to lead and can bring it home on their clothes when they work in auto repair, mining, pipe fitting, battery manufacturing, painting, construction and certain other fields

You're sneezing, coughing, and all stuffed up. It sounds and feels like a cold, alright. But as time goes on, you start to wonder. Is it turning into a sinus infection? They've got some things in common, but there are ways to tell them apart. The right ID lets your doctor get you the best treatment. What Is a Common Cold? It's an infection caused by a virus, a tiny living thing. You can't miss the symptoms: Nasal congestion Runny nose Post-nasal drip (drop-by-drop release of fluid from your nose into the back of the throat) Headache Fatigue You may also get a cough and a mild fever. The symptoms usually build, peak, and slowly disappear. Some medications can ease symptoms. For example, decongestants may decrease drainage and open the nasal passages. Pain relievers may help with fever and headache. Cough medicine may help, as well. Colds typically last from a few days to about a week or longer. Sometimes, a cold may cause swelling in the sinuses, hollow spaces in your skull that are connected to each other. The swelling can prevent the flow of mucus.

Euthyroid sick syndrome (ESS), sick euthyroid syndrome (SES), thyroid allostasis in critical illness, tumours, uremia and starvation (TACITUS), non-thyroidal illness syndrome (NTIS) or low T3 low T4 syndrome is a state of adaptation or dysregulation of thyrotropic feedback control where the levels of T3 and/or T4 are ...
