- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
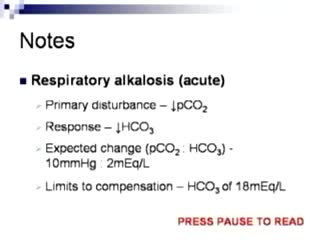
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Arterial Blood Gas Sampling


Loyola Full Male Exam Part 2 A video from Loyola medical school, Chicago showing the full examination of the male
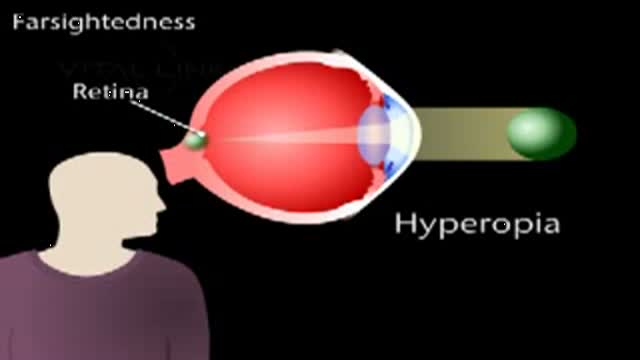
This animated video reviews hyperopia, or farsightedness.
Embolization is a medical advance that shrinks uterine fibroids. One tiny incision allows us to solve the problem quickly, safely and without surgery

his patient had spilled boiling water on his lower leg a couple days before. This isn't complicated but the teaching points should focus on draining the large blistered areas and attempting to maintain moisture as long as we can so the skin doesn't contract down on itself.

The examination room should be quiet, warm and well lit. After you have finished interviewing the patient, provide them with a gown (a.k.a. "Johnny") and leave the room (or draw a separating curtain) while they change. Instruct them to remove all of their clothing (except for briefs) and put on the gown so that the opening is in the rear. Occasionally, patient's will end up using them as ponchos, capes or in other creative ways. While this may make for a more attractive ensemble it will also, unfortunately, interfere with your ability to perform an examination! Prior to measuring vital signs, the patient should have had the opportunity to sit for approximately five minutes so that the values are not affected by the exertion required to walk to the exam room. All measurements are made while the patient is seated. Observation: Before diving in, take a minute or so to look at the patient in their entirety, making your observations, if possible, from an out-of-the way perch. Does the patient seem anxious, in pain, upset? What about their dress and hygiene? Remember, the exam begins as soon as you lay eyes on the patient. Temperature: This is generally obtained using an oral thermometer that provides a digital reading when the sensor is placed under the patient's tongue. As most exam rooms do not have thermometers, it is not necessary to repeat this measurement unless, of course, the recorded value seems discordant with the patient's clinical condition (e.g. they feel hot but reportedly have no fever or vice versa). Depending on the bias of a particular institution, temperature is measured in either Celcius or Farenheit, with a fever defined as greater than 38-38.5 C or 101-101.5 F. Rectal temperatures, which most closely reflect internal or core values, are approximately 1 degree F higher than those obtained orally. Respiratory Rate: Respirations are recorded as breaths per minute. They should be counted for at least 30 seconds as the total number of breaths in a 15 second period is rather small and any miscounting can result in rather large errors when multiplied by 4. Try to do this as surreptitiously as possible so that the patient does not consciously alter their rate of breathing. This can be done by observing the rise and fall of the patient's hospital gown while you appear to be taking their pulse. Normal is between 12 and 20. In general, this measurement offers no relevant information for the routine examination. However, particularly in the setting of cardio-pulmonary illness, it can be a very reliable marker of disease activity. Pulse: This can be measured at any place where there is a large artery (e.g. carotid, femoral, or simply by listening over the heart), though for the sake of convenience it is generally done by palpating the radial impulse. You may find it helpful to feel both radial arteries simultaneously, doubling the sensory input and helping to insure the accuracy of your measurements. Place the tips of your index and middle fingers just proximal to the patients wrist on the thumb side, orienting them so that they are both over the length of the vessel.
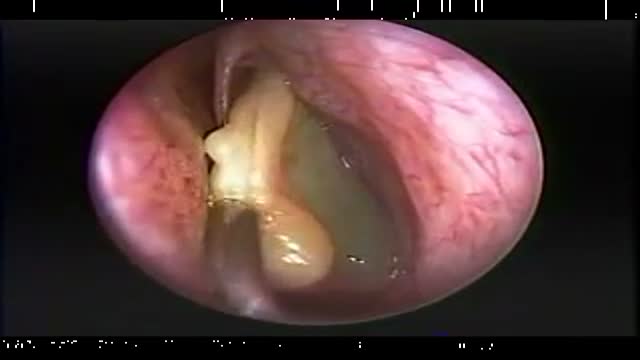
Endoscopic Nasal Polypectomy

#ComprehensiveClinicalClass
History, Examination and Management of Hernia
Mentor: Dr. Nishanth, Consultant Surgeon, Bengaluru.
THE WHITE ARMY
To make studies more interesting and enjoyable, we are constantly trying to share most important tables, charts, diagrams, mnemonics, scoring systems, diagnostic criterias, motivating quotes and other useful study materials on
ANDROID APP - All in 1 Free Medical Education App for Medicos
https://play.google.com/store/....apps/details?id=com.
INSTAGRAM PAGE
@the_whitearmy
https://www.instagram.com/the_whitearmy/
TELEGRAM GROUP
PDFs, PPTs and other study materials stored for easy, convenient access and download.
https://t.me/whitearmyofmedicos
Anyone interested to present clinical cases, willing to join whatsapp discussion group, can send a mail to whitearmyofmedicos@gmail.com
#StudyManiaInSocialMedia
#HelpOthersToHelpOurselves
#StudyEnjoyingEnjoyStudying
DISCLAIMER
THE WHITE ARMY does not own or claim to own any of the media used in the following video/stream. The media belong to their respective owners who may have copyright over them.The media have been taken from various sources and are used for medical educational purposes only. The following video/stream may contain images that may not be suitable for all audiences, viewer discretion is advised.
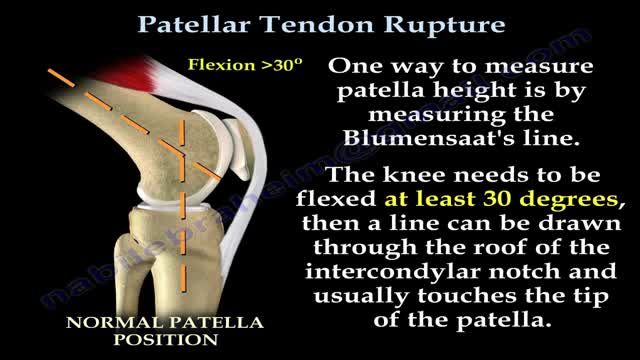
Patellar tendon rupture is a rupture of the tendon that connects the patella to the tibia. The superior portion of the patellar tendon attaches on the posterior portion of the patella, and the posterior portion of the patella tendon attaches to the tibial tubercle on the front of the tibia.
Some common signs of spinal tumors may include the following: Pain (back and/or neck pain, arm and/or leg pain) Muscle weakness or numbness in the arms or legs. Difficulty walking. General loss of sensation. Difficulty with urination (incontinence) Change in bowel habits (retention) Paralysis to varying degrees.

Dr. Nick demonstrates how to numb a toe for a patient who had a subungual hematoma “collection of blood under the nail”. This patient stubbed his toe and needed to have the nail removed.
#satisfying #reaction #amazing
MAKE SURE TO SUBSCRIBE FOR ALL THE NEW SURGICAL AND EDUCATIONAL VIDEOS COMING!!
👉🏻For more information visit :
https://drnickcampi.com
👉🏻Follow me on TikTok!!
https://vm.tiktok.com/ZMeXLbc5F/I’ll
👉🏻Connect with me!!
https://www.instagram.com/drnickcampitelli
👉🏻Check out this video of how we remove an ingrown toenail!
https://youtu.be/JyZo8aZDYds
👉🏻Dr. Nick Campitelli Performs latest Minimally Invasive Bunion Surgery! Watch this video!
https://youtu.be/eRpABMsCbOU
Dr. Nick Campitelli is a podiatrist who specializes in foot and ankle surgery in the Akron and Cleveland Ohio area. He is the Residency Director of the Western Reserve Hospital / University Hospital Podiatric Medicine and Surgery Residency Program.
*** All content found on the this YouTube video including: text, images, audio, or other formats were created for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you heard on this video. ***
◦

Shoulder Clinical Examination - Medical School Clinical Skills - Dr Gill
Personally, I find the shoulder examination the most complex examination possibly as there are so many variations and special tests. Some of which overlap and some will relate specifically to a patients presentation.
Often in a medical school syllabus, only select special tests will be used. In this shoulder exam demonstration, we include the Hawkins-Kennedy Test looking for impingement. This is dovetailed with examination for bicipital tendonitis as this is another possible cause of impingement type symptoms.
This shoulder upper limb exam follows the standard "Look, Feel, Move" orthopaedic exam approach, and overall order as set out in MacLeods Clinical Examination
Watch further orthopaedic examinations for your OSCE revision:
The Spine Examination:
https://youtu.be/pJxMHa6SCgU
Knee Examination
https://youtu.be/oyKH4EYfJDM
Hip Joint Clinical Examination
https://youtu.be/JC9GKq5nSdQ
________
Please note that there is no ABSOLUTE way to perform a clinical examination. Different institutions and even clinicians will have differing degrees of variations - the aim is the effectively identify medically relevant signs.
However during OSCE assessments. Different medical schools, nursing colleges, and other health professional courses will have their own preferred approach to a clinical assessment - you should concentrate on THEIR marks schemes for your assessments.
The examination demonstrated here is derived from Macleods Clinical Examination - a recognized standard textbook for clinical skills.
#ShoulderExamination #ClinicalSkills #DrGill

Barrett's esophagus is a complication of chronic (long lasting) and usually severe gastrointestinal reflux disease (GERD), but occurs in only a small percentage of patients with GERD. Criteria are needed for screening patients with GERD for Barrett's esophagus. Until validated criteria are available, it seems reasonable to do screening endoscopies in GERD patients who cannot be taken off acid suppression therapy after two to three years. The diagnosis of Barrett's esophagus rests upon seeing (at endoscopy) a pink esophageal lining that extends a short distance (usually less than 2.5 inches) up the esophagus from the gastroesophageal junction and finding intestinal type cells (goblet cells) on biopsy of the lining. There is a small but definite increased risk of cancer of the esophagus (adenocarcinoma) in patients with Barrett's esophagus.

The most common symptoms of infection from animal bites are redness, pain, swelling, and inflammation at the site of the bite. You should seek immediate medical treatment if any of these symptoms continue for more than 24 hours. Other symptoms of infection include: pus or fluid oozing from the wound

Drainage of Pus from a Dental Abscess

If your knee is severely damaged by arthritis or injury, it may be hard for you to perform simple activities, such as walking or climbing stairs. You may even begin to feel pain while you are sitting or lying down. If nonsurgical treatments like medications and using walking supports are no longer helpful, you may want to consider total knee replacement surgery. Joint replacement surgery is a safe and effective procedure to relieve pain, correct leg deformity, and help you resume normal activities. Knee replacement surgery was first performed in 1968. Since then, improvements in surgical materials and techniques have greatly increased its effectiveness. Total knee replacements are one of the most successful procedures in all of medicine. According to the Agency for Healthcare Research and Quality, more than 600,000 knee replacements are performed each year in the United States. Whether you have just begun exploring treatment options or have already decided to have total knee replacement surgery, this article will help you understand more about this valuable procedure.

Problems that affect ovulation, and the hormones involved with ovulation, are the most common cause of female infertility. They include: Polycystic Ovarian Syndrome (PCOS). Women with PCOS do not ovulate regularly and they experience infrequent or absent menstrual cycles.


Your baby's sex is set at conception. At around 7 weeks, your baby's internal sex organs – such as ovaries and testes – begin to form in the abdomen. Male and female sex organs and genitalia look the same at this stage because they're derived from the same structures. At around 9 weeks, boys and girls begin to develop differently. In girls, a tiny bud emerges between the tissue of the legs. This bud will become the clitoris. The membrane that forms a groove below the bud separates to become the labia minora and the vaginal opening. By 22 weeks, the ovaries are completely formed and move from the abdomen to the pelvis. They already contain a lifetime supply of 6 million eggs. In boys, the bud develops into the penis and starts to elongate at around 12 weeks. The outer membrane grows into the scrotal sac that will later house the testicles. By 22 weeks, the testes have formed in the abdomen. They already contain immature sperm. Soon they'll begin their descent to the scrotum, but it's a long journey. They'll reach their destination late in pregnancy, or for some boys, after birth. If you're eager to find out whether you're having a girl or a boy, you'll have to wait until you're at least 17 weeks pregnant. That's when the genitals have developed enough to be seen on an ultrasound.
