- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
In caring for patients who are critically ill, access to the central venous circulation is important. Central venous access allows the placement of various types of intravenous (IV) lines to facilitate the infusion of fluids, blood products, and drugs and to obtain blood for laboratory analysis. It is also an essential procedure in patients in whom placement of a line in a peripheral vein is impossible. A central line may be the only means of venous access in such cases.
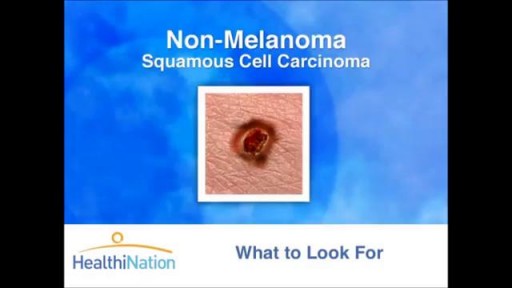
The Skin Cancer Foundation, founded in 1979 by dermatologist and Mohs surgeon Perry Robins, MD, is a global organization solely devoted to educating the public and medical community about skin cancer prevention, early detection, and treatment

This video demonstrates how a broken nose is fixed using only local anesthesia and without sedation. Of course, this can also be performed while asleep.

Sporotrichosis (also known as "rose gardener's disease") is a disease caused by the infection of the fungus Sporothrix schenckii. This fungal disease usually affects the skin, although other rare forms can affect the lungs, joints, bones, and even the brain.
High blood pressure and high cholesterol are the most common causes of these spasms. Approximately 2 percent of people with angina, or chest pain and pressure, experience coronary artery spasms. Coronary artery spasms can also occur in people who have atherosclerosis.
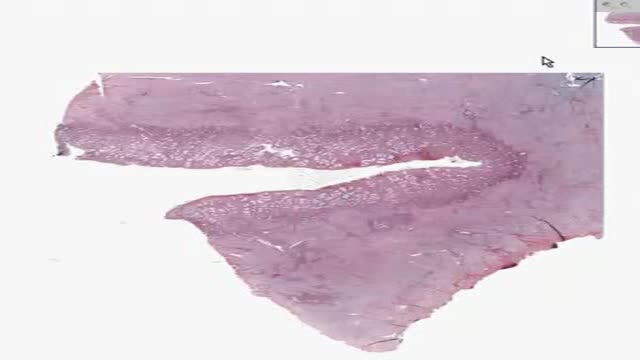
Histology of Secretory Endometrium

Unstable ankle joints after internal fixation of type B malleolar fractures exist. Residual instability most often occurs after trimalleolar fractures with initial joint dislocation. Treatment with an additional positioning screw generally produced a satisfactory result.

Cancer starts when cells in a part of the body begins to grow out of control and can spread to other areas of the body. There are many kinds of cancer. Cells in nearly any part of the body can become cancer. To learn more about how cancers start and spread, see What Is Cancer? Leukemias are cancers that start in cells that would normally develop into different types of blood cells. Here we will talk about acute myeloid leukemia (AML). Acute myeloid leukemia (AML) has many other names, including acute myelocytic leukemia, acute myelogenous leukemia, acute granulocytic leukemia, and acute non-lymphocytic leukemia. “Acute” means that this leukemia can progress quickly if not treated, and would probably be fatal in a few months. “Myeloid” refers to the type of cell this leukemia starts from. Most cases of AML develop from cells that would turn into white blood cells (other than lymphocytes), but some cases of AML develop in other types of blood-forming cells. The different types of AML are listed in “ How is acute myeloid leukemia classified?” AML starts in the bone marrow (the soft inner part of certain bones, where new blood cells are made), but in most cases it quickly moves into the blood. It can sometimes spread to other parts of the body including the lymph nodes, liver, spleen, central nervous system (brain and spinal cord), and testicles. Other types of cancer can start in these organs and then spread to the bone marrow. But these cancers that start elsewhere and then spread to the bone marrow are not leukemias. Normal bone marrow, blood, and lymphoid tissue To understand the different types of leukemia, it helps to know about the blood and lymph systems.
Is there scientific proof we can heal ourselves?

Work out the length of your average menstrual cycle. Day one is the first day of the menstrual period and the last day is the day before the next period begins. Ovulation happens about two weeks before the next expected period. So if your average menstrual cycle is 28 days, you ovulate around day 14.

Blepharitis is an inflammation of the eyelids in which they become red, irritated and itchy and dandruff-like scales form on the eyelashes. It is a common eye disorder caused by either bacteria or a skin condition, such as dandruff of the scalp or acne rosacea. It affects people of all ages. Although uncomfortable, blepharitis is not contagious and generally does not cause any permanent damage to eyesight.

Rheumatic heart disease (RHD) is the most common acquired heart disease in children in many countries of the world, especially in developing countries. The global burden of disease caused by rheumatic fever currently falls disproportionately on children living in the developing world, especially where poverty is widespread. RHD is a chronic heart condition caused by rheumatic fever that can be prevented and controlled. Rheumatic fever is caused by a preceding group A streptococcal (strep) infection. Treating strep throat with antibiotics can prevent rheumatic fever. Moreover, regular antibiotics (usually monthly injections) can prevent patients with rheumatic fever from contracting further strep infections and causing progression of valve damage. Consequences of rheumatic heart disease Acute rheumatic fever primarily affects the heart, joints and central nervous system. The major importance of acute rheumatic fever is its ability to cause fibrosis of heart valves, leading to crippling valvular heart disease, heart failure and death. The decline of rheumatic fever in developed countries is believed to be the result of improved living conditions and availability of antibiotics for treatment of group A streptococcal infection. Overcrowding, poor housing conditions, undernutrition and lack of access to healthcare play a role in the persistence of this disease in developing countries.

What is Esophageal Dilation?Esophageal dilation is a procedure that allows your doctor to dilate, or stretch, a narrowed area of your esophagus [swallowing tube]. Doctors can use various techniques for this procedure. Your doctor might perform the procedure as part of a sedated endoscopy. Alternatively, your doctor might apply a local anesthetic spray to the back of your throat and then pass a weighted dilator through your mouth and into your esophagus. Why is it Done? The most common cause of narrowing of the esophagus, or stricture, is scarring of the esophagus from reflux of acid occurring in patients with heartburn.

This 25 year young female wanted her split earlobe hole to be repaired.Ear lobe ring hole usually elongated due to continuous use of fancy heavy ear rings.most young ladies suffer from this problem, subsequently this get converted to complete split ear lobe.This needs surgical repair only.This is a cosmetic repair .watch the video , how this repair is done.Usually the split is completely closed with suture.After healing new hole to be done little distance from the repair site.
Bone pain: Pain is the most common sign of bone cancer, and may become more noticeable as the tumor grows. Bone pain can cause a dull or deep ache in a bone or bone region (e.g., back, pelvis, legs, ribs, arms). Early on, the pain may only occur at night, or when you are active.
Multiple sclerosis (MS) is a potentially disabling disease of the brain and spinal cord (central nervous system). In MS, the immune system attacks the protective sheath (myelin) that covers nerve fibers and causes communication problems between your brain and the rest of your body. Eventually, the disease can cause the nerves themselves to deteriorate or become permanently damaged. Signs and symptoms of MS vary widely and depend on the amount of nerve damage and which nerves are affected. Some people with severe MS may lose the ability to walk independently or at all, while others may experience long periods of remission without any new symptoms. There's no cure for multiple sclerosis. However, treatments can help speed recovery from attacks, modify the course of the disease and manage symptoms

How to memorize more in pharma: Drug names, dental implications, numbers

The purpose of the organs of the male reproductive system is to perform the following functions: To produce, maintain, and transport sperm (the male reproductive cells) and protective fluid (semen) To discharge sperm within the female reproductive tract during sex To produce and secrete male sex hormones responsible for maintaining the male reproductive system
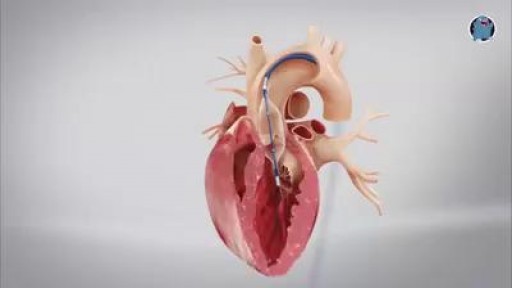
This minimally invasive surgical procedure repairs the valve without removing the old, damaged valve. Instead, it wedges a replacement valve into the aortic valve’s place. The surgery may be called a transcatheter aortic valve replacement (TAVR) or transcatheter aortic valve implantation (TAVI). Valve-within-valve — How does it work? Somewhat similar to a stent placed in an artery, the TAVR approach delivers a fully collapsible replacement valve to the valve site through a catheter. Once the new valve is expanded, it pushes the old valve leaflets out of the way and the tissue in the replacement valve takes over the job of regulating blood flow.

AirXpanders Inc. designs, manufactures and distributes the revolutionary AeroFormTM Patient Controlled Tissue Expander. A first for women who choose reconstructive surgery following a mastectomy, the AeroForm tissue expander does not use intrusive and painful saline injections via syringe needles. The AeroForm patient controlled tissue expander utilizes a needle-free inflation system via a patient-controlled handheld device, which releases specified amounts of air in the form of carbon dioxide
