- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

http://control-blood-sugar.good-info.co Low Blood Sugar, Signs Of Low Blood Sugar, Low Iron In Blood, Normal Glucose Levels In Blood Are You Suffering From High Or Uncontrollable Blood Sugar? Because This May Be The Solution. If you’re one of the 387 million people in the world trying to win the battle against uncontrollable blood sugar or even diabetes. Then you’re in the right place, as believe it or not, these conditions can be completely reversed from the comfort of your own home in just 3 short weeks. Are you. Tired of poking your skin with expensive needles everyday? Tired of dealing with the constant lethargy and lack of energy that’s associated with your uncontrollable blood sugar? Tired of living your life with stubborn body fat on your waist, legs,and thighs? Tired of being embarrassed to go to the beach or even taking your shirt off in front of your kids? Tired of waking up with a headache in a soaked bed from sweating so much at night? If you are sick and tired of these all of these conditions and more, then I am happy to tell you that all these conditions of your uncontrollable blood sugar can be completely thrown away for good! click here. http://control-blood-sugar.good-info.co


Insight eNO has revolutionized asthma treatment. Apieron’s asthma products as shown in this demo in AARC (American Association for Respiratory Care)help in managing asthma for patients suffering from acute asthma attacks by detecting exhaled nitric oxide (eNO) present in the human breath.
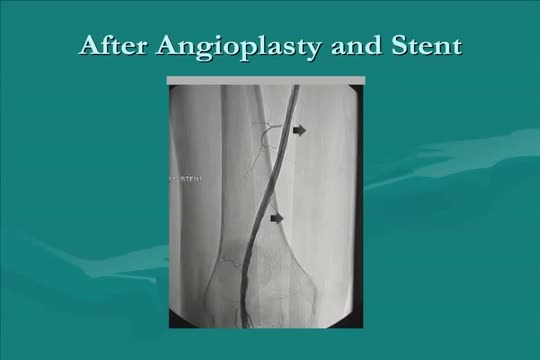
Roman Nowygrod, MD, a surgeon at NewYork-Presbyterian/Columbia University Medical Center, explains the different surgical approaches to treat Peripheral Arterial Disease (PAD).

Professional breast exam

Although the success rate of dental implant is very high, there are about 10% of failure in all dental implantation. The cause is usually related to the bone quality of the implant site. Once the implant failed, it can be easily removed, wait for 6 weeks and re-implant again. It is easier to remove a failed implant than a natural tooth.

Devi Shetty, founder of Narayana Health in India, reflects on the remarkable fact that, after 26 years of operation, the cost of heart surgery at Narayana Health has come down dramatically, and shares some of the strategies used to maintain high quality with low patient cost.
Learn more about the Creating Emerging Markets Project and explore its many compelling interviews: https://www.hbs.edu/creating-e....merging-markets/Page

Delorme Operation for Rectal Prolapse

Ear Examination ENT is often a challenging examination, crossing over with the cranial nerve examination of the vestibular cochlear exam as well at other neurological assessments of balance
Here we will review the ear examination, looking both at the use of the otoscope, but also the Dix-Hallpike Manoeuvre, along with HINTS assessment. the Webers and Rinne's test is also included to determine types of hearing loss.
Often these ear examination techniques are performed separately, depending on the patients presenting complaint
#EARExamination #DrGill #ClinicalSkills
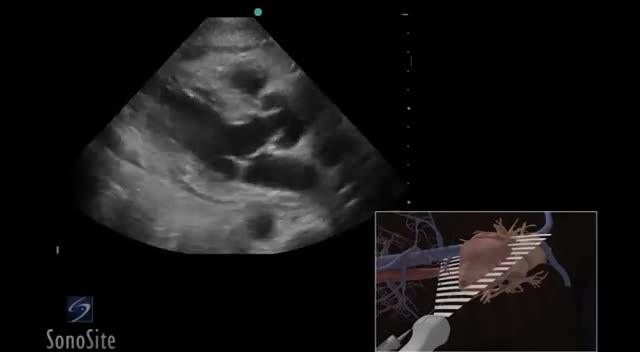
Using 3D animations we have come up with a new way of demonstrating how to perform portable ultrasound examinations
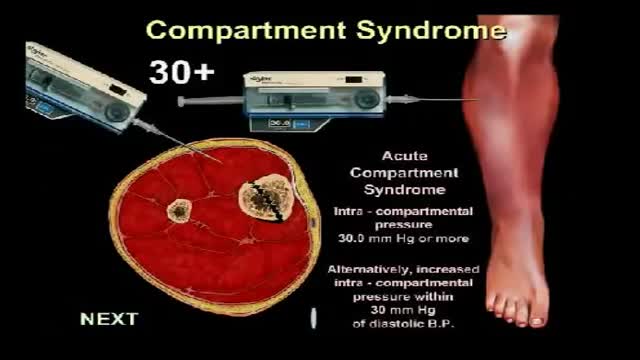
Acute compartment syndrome refers to ischemic tissue damage secondary to elevated pressures in the enclosed compartments of the lower legs or forearm. When the tissue pressure in an enclosed compartment exceeds the perfusion pressure, the resulting diminished tissue perfusion and compromised blood flow to the muscles and nerves inevitably lead to ischemic tissue necrosis. Majority of the cases involving the lower extremities are due to a traumatic event, most commonly tibial fractures. Other causes include a crush injury or other long bone fractures in a motor vehicle accident, a tight cast or dressing after trauma, and drug overdose.

Watch that video to know the op 10 Signs of Ovulation in Women

Nosebleeds are common due to the location of the nose on the face, and the large amount of blood vessels in the nose. The most common causes of nosebleeds are drying of the nasal membranes and nose picking (digital trauma), which can be prevented with proper lubrication of the nasal passages and not picking the nose.

METHODS:
Previously existing methods are characterized by unpleasant scars that, despite surgeons promises, remain for life.
Incisions are:
- around the areola (Round block) leading to a flat areola, often unpleasant hypertophic skars, skin rippling.
- inverted T (around the areola, vertically down and in the fold under the breast).
- Vertical (around the areola and vertically down). Due to the extess skin, incisions often turn into inverted L or T. Rearrangement of glandular tissue and skin changes the shape of the breasts and may be different from expectations. Scars worry patients and sometimes cause disturbances in the relationship with their partner.
- No scars. The "Serdev Suture" lifting technique for breast lifting without scars (only points - needle perforations in the skin) is created by the Bulgarian cosmetic surgeon Prof. Dr. Nikolay Serdev. It is a novelty that had changed the cosmetic surgery world in the last 10-14 years for young patients. The technique is especially important in Asia and Latin America, for Asians, African-Americans, Indians, and others who form keloids and lumpy scars after operations.
The Serdev suture method can achieve lift upto and over 14 centimeters and is most suitable for the following types of breasts:
- not very heavy full breasts.
- in the presence of subpectoral implants with subsequent drooping of the breasts after childbirth and lactation.
- empty and loose breasts after childbirth and breastfeeding. In such cases this technique is combined with subpectoral implants. In sagging breasts implants should not be placed in the skin over the pectoral muscles, because thus will lead to even more drooping. Therefore, breast lift requires breast fixation to the level of the pectoral muscle (the normal position in young women), and then placement of appropriate implants under the muscle, to hold them in the appropriated position.
- in drooping breasts after subglandular augmentation (over the muscle). In such cases, patients should not wait until the skin elongation becomes visible. The implants should be removed, the capsule removed - a difficult but a necessary operation, preventing postop seromas and infection. Implants should be placed under the pectoralis muscle to wear them. Patients should orient the cosmetic surgeon at what level they want the nipples - in the middle of the implant, higher or lower.
Implants should be generally replaced - below the muscle implants should be smooth, move naturally without hurting the muscle.
Because of modern anesthetics and new methods without trauma, pain and swelling after surgery are not significant. In 3-4 days, patients can return to social life, even the next day, but it is preferable to rest for 2-3 days.
Exercises with the arms and weight lifting is prohibited for a month and a half.
Due to lack of scars, the breast lift using the Serdev sutures can be repeated to maintain the aesthetic appearence of the breasts even in advanced age.
Gigantomastia i.e. very large, very heavy and drooping breasts can not be operated in this manner, because of gravity and overskin.
Early mastopexy using Serdev sutures is recommended before too much changes in the tissues. If late, more and more complex interventions are required.
"A lot of people are opting for various breast procedures and one of the most common among them is “mastopexy”. This is the surgery that involved uplifting of sagging breasts and, in certain cases, repositioning of the nipple and areola in order to restore normality and beauty. The excess skin is removed and firmness is provided to the breasts. Though mastopexy can be done as a stand alone surgery, many people combine it with breast augmentation which involves inserting implants inside the b
Understand how this world-class surgery platform operates a minimally invasive robotic surgery during a medical procedure for prostate cancer.
Acute sinusitis can be triggered by a cold or allergies and may resolve on its own. Chronic sinusitis lasts up to eight weeks and may be caused by an infection or growths. Symptoms include headache, facial pain, runny nose, and nasal congestion. Acute sinusitis usually doesn't require any treatment beyond symptomatic relief with pain medications, nasal decongestants, and nasal saline rinses. Chronic sinusitis may require antibiotics.

Vaginoplasty is any surgical procedure that results in the construction or reconstruction of the vagina. It is a type of genitoplasty. Pelvic organ prolapse is often treated with one or more surgeries to repair the vagina.

Watch that Female Genital Walls Tightening Plastic Surgery
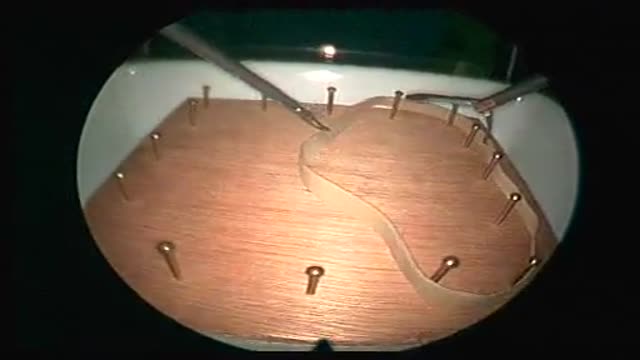
This task requires streching a rubber band around 16 nails on a wooden board. A penalty is calculated when the rubber band is not streched around a nail at the end of the task. Score = time (seconds) + number of missed nails x 10. Performance standard: Score = 62 sec [Kolkman 2008]
Access to processes within the skull base with lateral extension to the pterygopalatine fossa are reached by combined subfrontal osteotomy and Le Fort I osteotomy
