- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

What's helping me become a better doctor

Zumba in Operation room
Adrenoleukodystrophy, or ALD, is a deadly genetic disease that affects 1 in 18 000 people. It most severely affects boys and men. This brain disorder destroys myelin, the protective sheath that surrounds the brain's neurons -- the nerve cells that allow us to think and to control our muscles.
Vertebrobasilar insufficiency is typically secondary to emboli, thrombi, or arterial dissection. The labyrinth and brainstem are commonly affected, and symptoms may include vertigo, dizziness, dysarthria, diplopia, and numbness.

Candida Albicans is more than just yeast- for most people, it's already mutated into a more aggressive fungal form that eats holes through the intestinal tract causing many of todays health problems like food allergies, autoimmune disorders, Crohn's disease, IBS, low energy and many more aggressive diseases. People need to know what it is and what to do about it.
Alpha-1 Antitrypsin Deficiency (Alpha-1) is a genetic (inherited) condition – it is passed from parents to their children through their genes. Alpha-1 may result in serious lung disease in adults and/or liver disease at any age.
Atrial fibrillation vs Atrial Flutter

Obesity is one of the most pervasive, chronic diseases in need of new strategies for medical treatment and prevention. As a leading cause of United States mortality, morbidity, disability, healthcare utilization and healthcare costs, the high prevalence of obesity continues to strain the United States healthcare system. Obesity is defined as excess adipose tissue. There are several different methods for determining excess adipose (fat) tissue; the most common being the Body Mass Index (BMI) (see below). A fat cell is an endocrine cell and adipose tissue is an endocrine organ. As such, adipose tissue secretes a number of products, including metabolites, cytokines, lipids, and coagulation factors among others. Significantly, excess adiposity or obesity causes increased levels of circulating fatty acids and inflammation. This can lead to insulin resistance, which in turn can lead to type 2 diabetes.

-The management of diaper rash includes frequent changing of diapers, avoiding tight-fitting diapers, exposing the skin to air, using diapers with super absorbent surfaces, and applying barrier creams such as zinc oxide or petrolatum.

Benzodiazepines are a class of agents that work on the central nervous system, acting selectively on gamma-aminobutyric acid-A (GABA-A) receptors in the brain. GABA is a neurotransmitter that inhibits or reduces the activity of nerve cells (neurons) within the brain. Benzodiazepines open GABA-activated chloride channels, and allow chloride ions to enter the neuron. This makes the neuron negatively charged and resistant to excitation.

The cause of pectus excavatum is not known however it can run in families, with up to 25 percent of affected patients reporting chest wall abnormalities in other family members. Pectus excavatum occurs in approximately 1 out of 400–1000 children and is three to five times more common in males than females.

An ileostomy is an opening in the belly (abdominal wall) that’s made during surgery. The end of the ileum (the lowest part of the small intestine) is brought through this opening to form a stoma, usually on the lower right side of the abdomen. A Wound Ostomy Continence nurse (WOCN or WOC nurse) or the surgeon will figure out the best location for your stoma. (A WOC nurse is a specially trained registered nurse who takes care of and teaches ostomy patients. This nurse may also be called an ostomy nurse.)
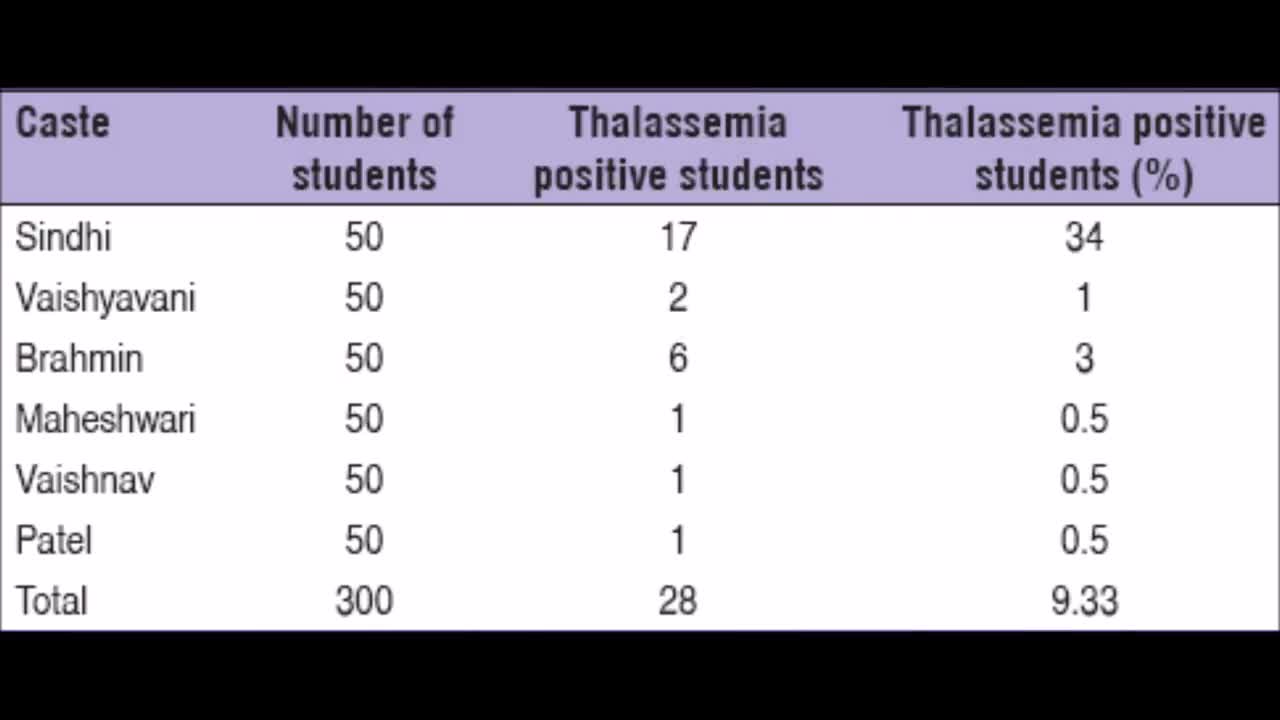
Thalassemia is a genetic blood disorder. People with Thalassemia disease are not able to make enough hemoglobin, which causes severe anemia. Hemoglobin is found in red blood cells and carries oxygen to all parts of the body. When there is not enough hemoglobin in the red blood cells, oxygen cannot get to all parts of the body. Organs then become starved for oxygen and are unable to function properly.

Coronary artery vasospasm, or smooth muscle constriction of the coronary artery, is an important cause of chest pain syndromes that can lead to myocardial infarction (MI), ventricular arrhythmias, and sudden death. It also plays a key role in the development of atherosclerotic lesions.Nov 22, 2016
A pneumothorax (noo-moe-THOR-aks) is a collapsed lung. A pneumothorax occurs when air leaks into the space between your lung and chest wall. This air pushes on the outside of your lung and makes it collapse. In most cases, only a portion of the lung collapses.
Niemann-Pick disease is a condition that affects many body systems. It has a wide range of symptoms that vary in severity. Niemann-Pick disease is divided into four main types: type A, type B, type C1, and type C2. These types are classified on the basis of genetic cause and the signs and symptoms of the condition. Infants with Niemann-Pick disease type A usually develop an enlarged liver and spleen (hepatosplenomegaly) by age 3 months and fail to gain weight and grow at the expected rate (failure to thrive). The affected children develop normally until around age 1 year when they experience a progressive loss of mental abilities and movement (psychomotor regression). Children with Niemann-Pick disease type A also develop widespread lung damage (interstitial lung disease) that can cause recurrent lung infections and eventually lead to respiratory failure. All affected children have an eye abnormality called a cherry-red spot, which can be identified with an eye examination. Children with Niemann-Pick disease type A generally do not survive past early childhood.
This animated video covers statins, fibrates, niacin, bile resins, and ezetimibe. We will discuss mechanisms of action, which part of the lipid profile is affected by each drug, and common side effects.
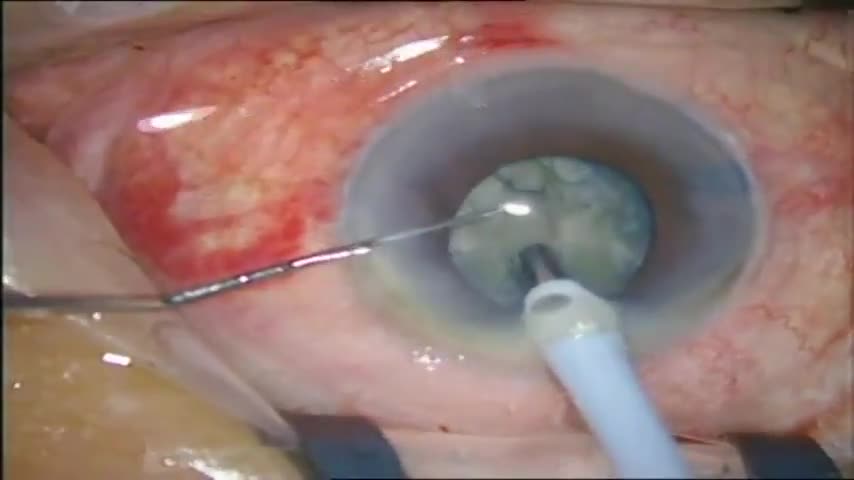
Stop and chop surgery on a hard cataract on a small pupil.

Cholecystectomy without General Anesthesia video
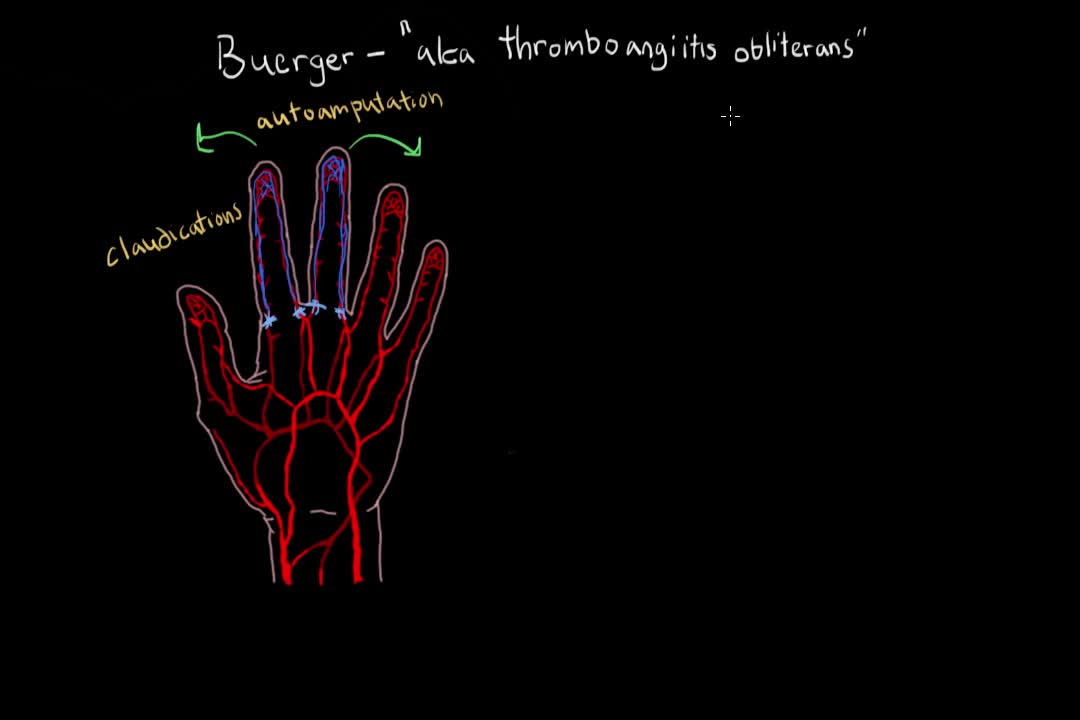
Buerger's disease (thromboangiitis obliterans) is a rare disease of the arteries and veins in the arms and legs. In Buerger's disease, your blood vessels become inflamed, swell and can become blocked with blood clots (thrombi). This eventually damages or destroys skin tissues and may lead to infection and gangrene. Buerger's disease usually first shows in your hands and feet and may eventually affect larger areas of your arms and legs. Virtually everyone diagnosed with Buerger's disease smokes cigarettes or uses other forms of tobacco, such as chewing tobacco. Quitting all forms of tobacco is the only way to stop Buerger's disease. For those who don't quit, amputation of all or part of a limb is sometimes necessary.
