- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Bizarre Body Modifications

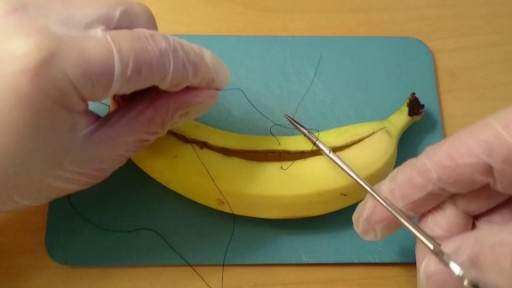
Learn How to Suture a Banana

A Big Size Fibrodenoma Removal Under Local Anesthesia




💥Patellar Tendon Pain AKA “Jumper’s Knee”👇
💥If you have this, it’s likely because your patellar tendon was over-stressed beyond what it can currently handle (due to loads that are too high or lack of recovery).
🔑 Try 5 reps of 45 second holds
🔑 2 min of rest in between each rep
🔑 Keep your knees at roughly 60 deg angle
🔑 7/10 intensity
🔑Should not increase pain during or after exercise
📚A research article found that this protocol using a knee extension machine provided significant short term pain relief. Most people don’t have a knee extension machine at home, so you could try out a wall sit instead!
🔑It may be useful during the season of competition to decrease pain and allow the athlete to compete, if needed.
❤️ Share this video with a friend who needs it!

This video shows you how to conduct a clinical examination of the shoulder and to identify common causes of pain.
This video clip is part of the FIFA Diploma in Football Medicine and the FIFA Medical Network. To enrol or to find our more click on the following link http://www.fifamedicalnetwork.com
The Diploma is a free online course designed to help clinicians learn how to diagnose and manage common football-related injuries and illnesses. There are a total of 42 modules created by football medicine experts. Visit a single page, complete individual modules or finish the entire course.
The network provides the opportunity for clinicians around the world to meet and share ideas relating to football medicine. Ask about an interesting case, debate current practice and discuss treatment strategies. Create a profile and log on to interact with other health professionals from around the globe.
This is not medical advice. The content is intended as educational content for health care professionals and students. If you are a patient, seek care of a health care professional.

Women's College Hospital is revolutionizing the way knee-replacement surgery is done. It is starting to provide the procedure as an ambulatory service. Patients can go home from hospital four hours after having the surgery. In some other hospitals knee replacement surgery patients have to stay as long as 4 days.
Read an excerpt from Theresa Boyle's story:
It’s been less than four hours since Greg Nemez underwent knee-replacement surgery and the 56-year-old Mississauga man is already on his way home from hospital.
This past Monday, he became the fifth patient at Toronto’s Women’s College Hospital to undergo the outpatient procedure, which normally requires a hospital stay of two or three days.
“I’m happy ... You have that freedom of movement from before. It’s like wow,” he said on the elevator as he was leaving the hospital.
After years of being unable to hold his leg straight, the real-estate agent can finally do so. A 20-year-old football injury had left him with severe arthritis and pain.
Read the full story:
https://www.thestar.com/news/g....ta/2018/04/11/he-got
Follow the Toronto Star on social media:
Facebook: https://www.facebook.com/torontostar/
Twitter: https://twitter.com/TorontoStar
Instagram: https://www.instagram.com/thetorontostar/

how to obtain intravenous access through cutting down over a large peripheral vein

Michael La Corte MD
Ped Card

how to to deal with fractures and dislocations

Utilizing specially engineered lasers, permanent hair removal has never been more comfortable for men and women of all colors and skin types. In just four or five sessions, patients can achieve lasting results without damaging the skin or any surrounding tissue.
Dark pigment (melanin) in the hair shaft and the papilla (the root of the hair follicle) are targeted by a specific light-energy emitted by the laser. In a tiny fraction of a second, the hair is simply vaporized without damaging the skin or any surrounding tissue.
In one pulse (that lasts a tiny fraction of a second) our lasers remove hair on a patch of skin the size of a quarter. The hair removal sensation is like plucking hair or getting snapped by a rubber-band. Our lasers incorporate a patented and state-of-the-art integrated cooling system that acts as a natural anesthetic, cooling down the skin to minimize any discomfort. Patients unanimously report that the hair removal treatment is a "piece of cake" compared to waxing.

Cricothyroidotomy NEJM

Part 3: from Loyola Medical School, Chicago showing clinical examination of the neurological system.

How to use a clamp?!

Sigmoid Colostomy
