- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Over 60 million Americans suffer from chronic heartburn. Get the basics on acid reflux
Third video about sarcoidosis. Please see my website for disclaimer.

LCHI - Hernia repair done by medical students with guidance and assistance of Professor Luiz Eduardo C. Miranda. Description of surgery is in portuguese.

the video will shed some light on congential lobar emphysema. Please visit my website for discliamer. www.academyofprofessionals.com

DMC Podiatrist Dr. Charles Kissel perfoms a bunionectomy to help a woman get back on her feet and back to work ~ Detroit Medical Center
Dr. Berger, Medical Director of Chapel Hill Tubal Reversal Center discusses the pros and cons of tubal reversal vs. IVF with a couple wanting a baby after a tubal ligation.

The video will shed light on mitral valve calcification. Please see disclaimer on my website. www.academyofprofessionals.com
Embospheres Microspheres are round particles which give them some extra advantages when they are used in embolization. This video gives a full idea about their advantages and use

Learn about electromagnetic navigation diagnostic bronchoscopy, a new technology used to diagnose small lung cancer tumors as small as a pencil eraser before they have the chance to spread. Cleveland Clinic physician Dr. Thomas Gildea demonstrates how this endobronchial ultrasound procedure, which involves using a small camera probe inserted thru the nose into the lungs, allows doctors to reach possible cancer in the lungs that they could never reliably get to before
USMLE Step 2 CS - Amenorrhea - This is just preview video. To get full access please visit our website : www.usmletutoring.com
H&E stain is a popular staining method in histology. Its a combination of two dyes: the basic dye (hematoxylin) and the alcohol-based dye (eosin). In an H&E stain you will usually see both eosinophilia and basophilia: the nuclei of cells basophilic (blue), while eosinophilia is typical of cytoplasmic constituents (pink). Xylene, alcohols, distilled water are also required.
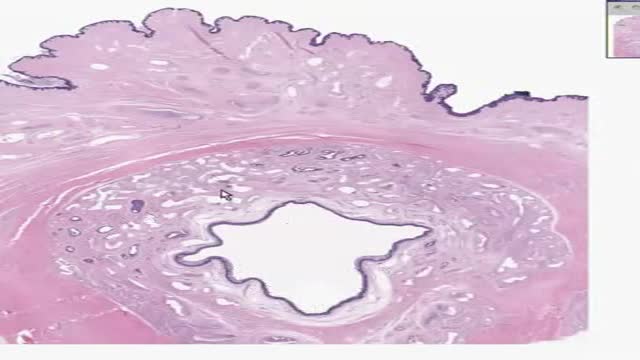
Histology of Male Urethra
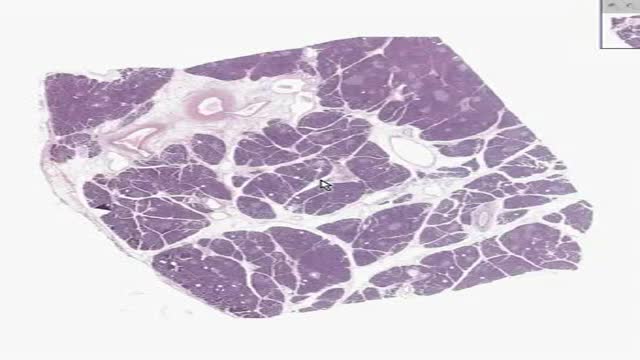
Histology of Pancreas
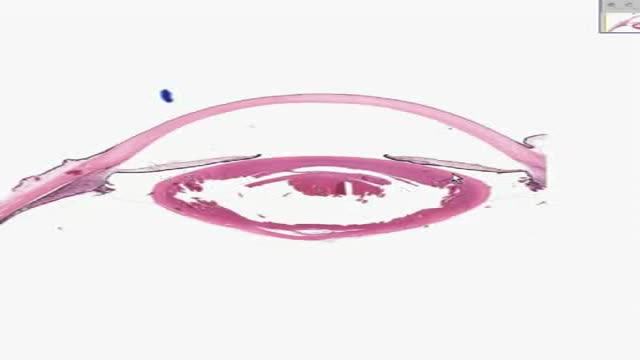
Histology of Eye
Surgical Mask How To Wear

AL EMADI HOSPITAL-QATAR-DOHA AMERICAN BOARD CERTIFICATE AESTHETIC MEDICINE

Coconut Oil Provides Thyroid Gland Benefits
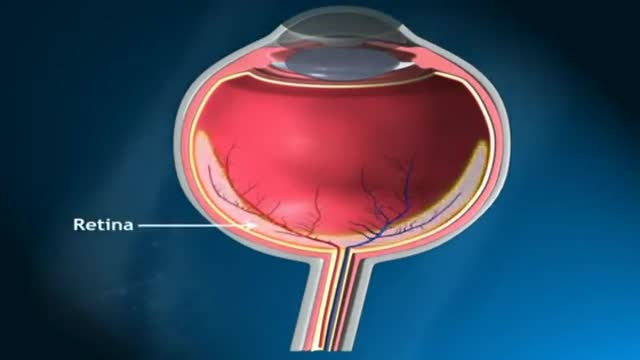
Glaucoma is called the silent thief of sight. It does not have symptoms during the early stages of the diseases and can make a patient blind over several years

This video goes through a case study of a 40 year old patient getting breast reduction surgery in NYC by board certified plastic surgeon Carlin Vickery of 5th Avenue Surgery located in New York, NY. For more information on this procedure please call our office at (212) 288-9800. This content is intended for general information only and does not replace the need for personal advice from a qualified health professional.
Cell Organelles in 3D
