- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

The most reliable clinical sign to detect ascites is checking for bilateral flank dullness. If a patient with ascites is lying supine, fluid accumulates in the flank regions, leading to dullness on percussion. At the same time, the air-filled bowel loops are forced upwards by the free fluid due to buoyancy, resulting in tympanitic percussion. To locate specifically where dullness shifts to tympany, or the air-fluid level, percussion should be performed from the sides towards the middle. To confirm that the dullness is caused by ascites, ask the patient to switch to a lateral decubitus position. If ascites is present, the air-filled bowel loops will shift accordingly and remain at the surface of the fluid. As a result, the air-fluid level will shift as well. This is known as shifting dullness.
Subscribe to AMBOSS YouTube for the latest clinical examination videos, medical student interviews, study tips and tricks, and live webinars!
Free 5 Day Trial: https://go.amboss.com/amboss-YT
Instagram: https://www.instagram.com/amboss_med/
Facebook: https://www.facebook.com/AMBOSS.Med/
Twitter: https://twitter.com/ambossmed
Blog: https://blog.amboss.com/us
#AMBOSSMed #ClinicalExamination

Watch that video of a Man With Pipe Penetrated His Head Inside Emergency Room

Delorme Operation for Rectal Prolapse

Ophthalmoscopy - Eye Clinical Examination - OSCE - Dr Gill
Direct Ophthalmoscopy use of the eyes is a very challenging clinical skill, incorporating both the examiner's knowledge of the retina, but also understanding the use of the ophthalmoscope
In this clinical skills tutorial, we look at the use of the direct ophthalmoscope as part of an ophthalmic examination
it should be noted that in the ideal circumstances, the room lights will be dimmed during the examination, and dilating eye drops used to improve the visualisation of the fundus
Some people may notice an ASMR effect from this clinical examination
#DrGill #Ophthalmoscopy #ClinicalSkills #EyeExam

Having trouble achieving a good night’s sleep? A few easy tips for your daily routine can help you get the rest you need.
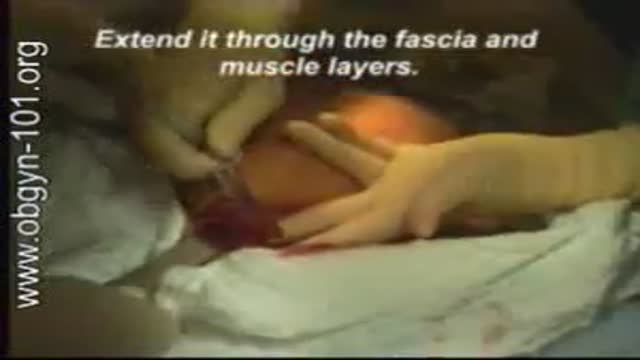
At one time, women who had delivered by cesarean section in the past would usually have another cesarean section for any future pregnancies. The rationale was that if allowed to labor, many of these women with a scar in their uterus would rupture the uterus along the weakness of the old scar. Over time, a number of observations have become apparent: Most women with a previous cesarean section can labor and deliver vaginally without rupturing their uterus. Some women who try this will, in fact, rupture their uterus. When the uterus ruptures, the rupture may have consequences ranging from near trivial to disastrous. It can be very difficult to diagnose a uterine rupture prior to observing fetal effects (eg, bradycardia). Once fetal effects are demonstrated, even a very fast reaction and nearly immediate delivery may not lead to a good outcome. The more cesarean sections the patient has, the greater the risk of subsequent rupture during labor. The greatest risk occurs following a “classical” cesarean section (in which the uterine incision extends up into the fundus.) The least risk of rupture is among women who had a low cervical transverse incision. Low vertical incisions probably increase the risk of rupture some, but usually not as much as a classical incision. Many studies have found the use of oxytocin to be associated with an increased risk of rupture, either because of the oxytocin itself, or perhaps because of the clinical circumstances under which it would be contemplated. Pain medication, including epidural anesthetic, has not resulted greater adverse outcome because of the theoretical risk of decreasing the attendant’s ability to detect rupture early. The greatest risk of rupture occurs during labor, but some of the ruptures occur prior to the onset of labor. This is particularly true of the classical incisions. Overall successful vaginal delivery rates following previous cesarean section are in the neighborhood of 70 This means that about 30of women undergoing a vaginal trial of labor will end up requiring a cesarean section. Those who undergo cesarean section (failed VBAC) after a lengthy labor will frequently have a longer recovery and greater risk of infection than had they undergone a scheduled cesarean section without labor. Women whose first cesarean was for failure to progress in labor are only somewhat less likely to be succesful in their quest for a VBAC than those with presumably non-recurring reasons for cesarean section. For these reasons, women with a prior cesarean section are counseled about their options for delivery with a subsequent pregnancy: Repeat Cesarean Section, or Vaginal Trial of Labor. They are usually advised of the approximate 70successful VBAC rate (modified for individual risk factors). They are counseled about the risk of uterine rupture (approximately 1in most series), and that while the majority of those ruptures do not lead to bad outcome, some of them do, including fetal brain damage and death, and maternal loss of future childbearing. They are advised of the usual surgical risks of infection, bleeding, anesthesia complications and surgical injury to adjacent structures. After counseling, many obstetricians leave the decision for a repeat cesarean or VBAC to the patient. Both approaches have risks and benefits, but they are different risks and different benefits. Fortunately, most repeat cesarean sections and most vaginal trials of labor go well, without any serious complications. For those choosing a trial of labor, close monitoring of mother and baby, with early detection of labor abnormalities and preparation for

A video showing the surgery of vaginal hysterectomy Operation

Have you ever swallowed something that wasn`t meant to be ingested?
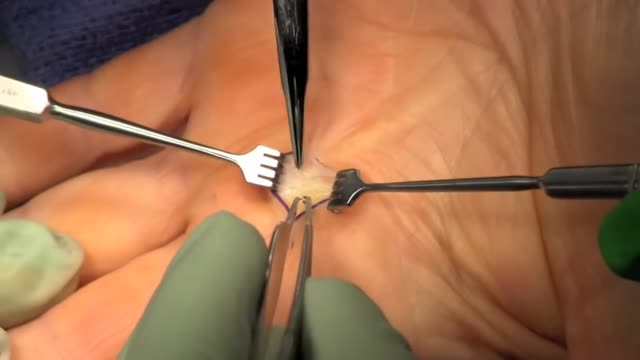
Trigger finger, also known as stenosing tenosynovitis (stuh-NO-sing ten-o-sin-o-VIE-tis), is a condition in which one of your fingers gets stuck in a bent position. Your finger may straighten with a snap — like a trigger being pulled and released. Trigger finger occurs when inflammation narrows the space within the sheath that surrounds the tendon in the affected finger. If trigger finger is severe, your finger may become locked in a bent position. People whose work or hobbies require repetitive gripping actions are at higher risk of developing trigger finger. The condition is also more common in women and in anyone with diabetes. Treatment of trigger finger varies depending on the severity.

Pulmonary fibrosis is a condition in which the tissue deep in your lungs becomes scarred over time. This tissue gets thick and stiff. That makes it hard for you to catch your breath, and your blood may not get enough oxygen. Causes of pulmonary fibrosis include environmental pollutants, some medicines, some connective tissue diseases, and interstitial lung disease. Interstitial lung disease is the name for a large group of diseases that inflame or scar the lungs. In most cases, the cause cannot be found. This is called idiopathic pulmonary fibrosis

a video of abdominal physical examination including all the required items:
-Inspection
-Palpation
-Percussion
-Auscultation

The baby will move head down if there is room or if there is tone in the support to the uterus to direct baby head down. Before 24-26 weeks most babies lie diagonal or sideways in the Transverse Lie position. Between 24-29 weeks most babies turn vertical and some will be breech.

They might not sound very life threatening, but a blood clot that develops in the deep veins of your leg, if left untreated and unable to dissolve of its own volition, may detach and travel to your lungs, causing a pulmonary embolism (or PE). In most cases, a leg blood clot will form due to lengthy periods of travel, for example if you remain immobile in cramped spaces—such as an airplane or bus—with few opportunities to stretch your legs or get up and walk around. Here are ten signs that you may have a dangerous blood clot in your leg

Misgav Ladach - Joel Cohen approach for breech presentation

Vial medication administration nursing skill. Learn techniques to withdraw medication from a vial using a syringe with a needle.
Medications can come in different forms, such as ampules, vials, tablets, capsules, and so forth. When withdrawing medication from a vial, there are a few things you'll want to know as a nursing student or nurse.
First, there are different needles that can be attached to the syringe. You can use a traditional needle with a beveled tip; you can use a blunt-tip needle to reduce the risk of needle sticks; or you can use a filter needle, which is sometimes required or recommended when drawing medication from a vial, particularly in cases of reconstituted medication.
When withdrawing from a vial, you'll want to do these things (assuming they fit with the protocols and manufacturer's instructions):
NOTE: Some medications or vaccines may require a different technique, so always consult with the manufacturer's instructions.
-gather your supplies
-perform hand hygiene
-clean the vial's top with alcohol prep
-attach the appropriate needle
-stick the needle using a technique to prevent coring of the rubber on the vial (start with 45 degree angle, and as you puncture the vial, rotate the needle to a 90 degree angle in one smooth motion).
-push air into the vial equal to the amount of medication you plan to draw
-invert the vial to withdraw medication
-remove air bubbles
-and much more
See more Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Notes: https://www.registerednursern.....com/how-to-withdraw-
Website: https://www.registerednursern.com/
More Videos: https://www.youtube.com/watch?v=R2XMro13dD0&list=UUPyMN8DzkFl2__xnTEiGZ1w
Nursing Gear: https://teespring.com/stores/registerednursern
Instagram: https://www.instagram.com/registerednursern_com/
Facebook: https://www.facebook.com/RegisteredNurseRNs
Twitter: https://twitter.com/NursesRN
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
FREE Nursing School Cheat Sheets at: http://www.NURSING.com
Get the full lesson on IM Injections here:
https://nursing.com/lesson/ski....lls-06-01-pill-crush
Check out our new Nurse Care Plan Lessons here:
https://bit.ly/3BPRfPL
Get Access to Thousands of Lessons here:
https://nursing.com/courses/
Welcome to the NURSING Family, we call it the most supportive nursing cohort on the planet.
At NURSING.com, we want to help you remove the stress and overwhelm of nursing school so that you can focus on becoming an amazing nurse.
Check out our freebies and learn more at: (http://www.nursing.com)
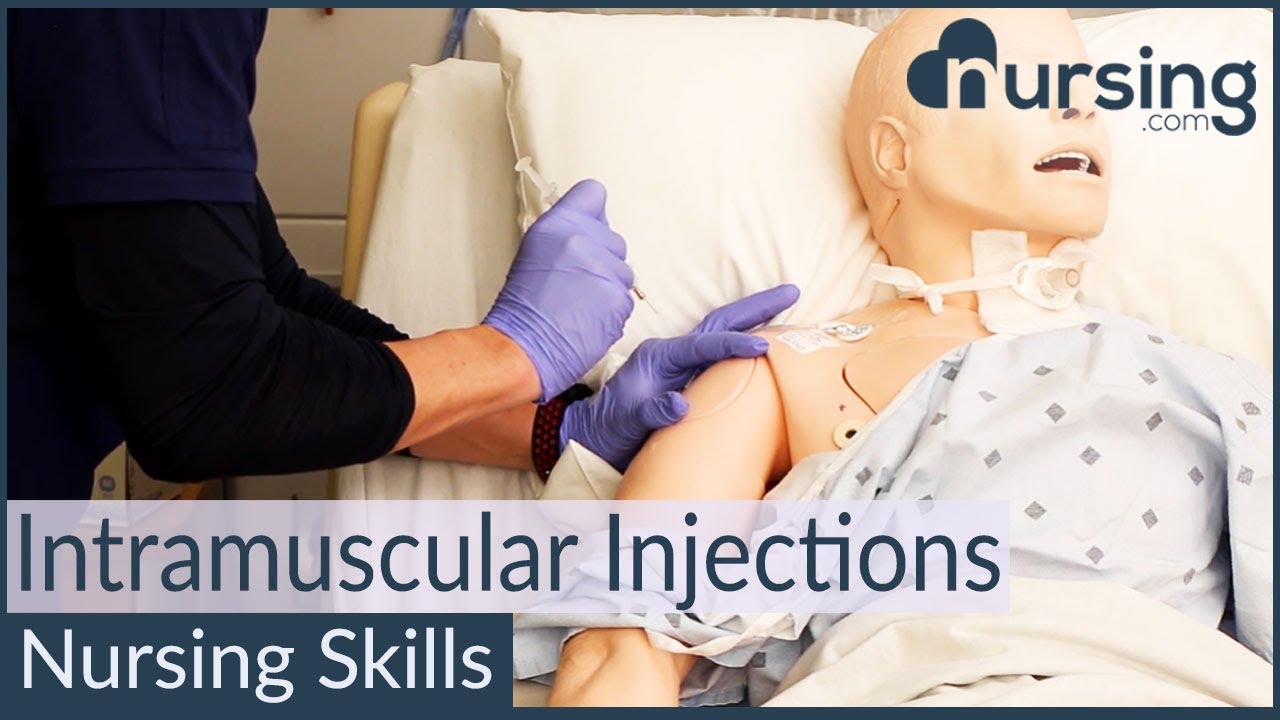
Intramuscular Injection Techniques (Nursing Skills)
In this video, we’re going to look at proper administration techniques for intramuscular medication administration. Of course, always follow your 5 rights and calculate the correct volume for administration. We love you guys! Go out and be your best selves today! And, as always, happy nursing!
Bookmarks:
0.05 Introduction to Intramuscular injections
0.16 site and needle selection
0.35 site sterilization
0.43 Z track method
0.58 needle insertion
1.10 medication injection
1.14 needle removal
1.25 bandaging and needle disposal
1.30 documentation and patient monitoring
1.35 Outro
Visit us at https://nursing.com/medical-disclaimer/ for disclaimer information.
NCLEX®, NCLEX-RN® are registered trademarks of the National Council of State Boards of Nursing, INC. and hold no affiliation with NURSING.com.

Twin Childbirth Video
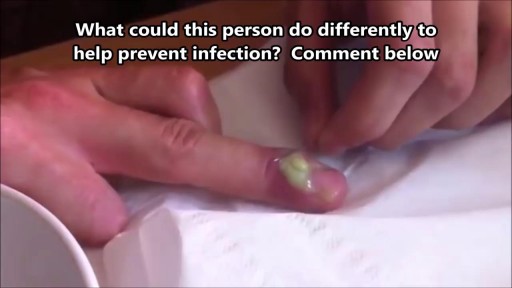
What Is a Paronychia (Nail Infection)? An infection that develops along the edge of the fingernail or toenail is called a paronychia (pear-ah-NIK-ee-ah). It is the most common hand infection and, if left untreated, can progress to a more severe infection of the entire finger or toe. Paronychia is distinguished from other infections such as onychomycosis and herpetic whitlow by its location and appearance.
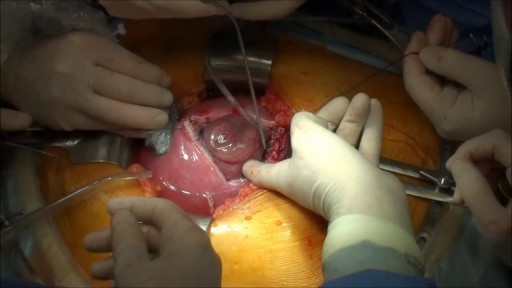
Prenatal repair of myelomeningocele (MMC), the most common and severe form of spina bifida, is a delicate surgical procedure where fetal surgeons open the uterus and close the opening in the baby's back while they are still in the womb.
Intra-Uterine Device IUD Removal
