- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
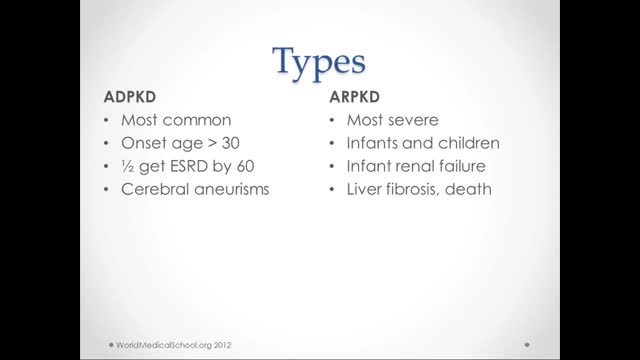
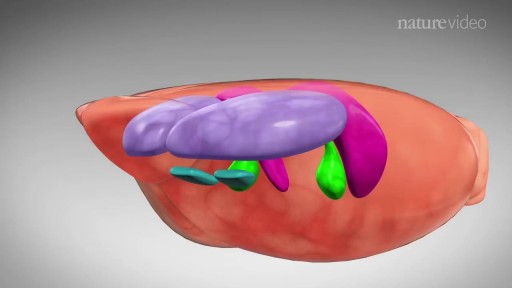
What is polycystic kidney disease? Polycystic kidney disease (also called PKD) causes numerous cysts to grow in the kidneys. These cysts are filled with fluid. If too many cysts grow or if they get too big, the kidneys can become damaged. PKD cysts can slowly replace much of the kidneys, reducing kidney function and leading to kidney failure. How common is PKD? In the United States about 600,000 people have PKD. It is the fourth leading cause of kidney failure. It is found in all races and occurs equally in men and women. It causes about 5% of all kidney failure. What other organs besides the kidney are affected by PKD? PKD can affect other organs besides the kidney. People with PKD may have cysts in their liver, pancreas, spleen, ovaries, and large bowel. Cysts in these organs usually do not cause serious problems, but can in some people. PKD can also affect the brain or heart. If PKD affects the brain, it can cause an aneurysm. An aneurysm is a bulging blood vessel that can burst, resulting in a stroke or even death. If PKD affects the heart, the valves can become floppy, resulting in a heart murmur in some patients. What are the clues that someone has PKD? Most people do not develop symptoms until they are 30 to 40 years old. The first noticeable signs and symptoms may include: Back or side pain An increase in the size of the abdomen Blood in the urine Frequent bladder or kidney infections High blood pressure High blood pressure is the most common sign of PKD. Occasionally, patients may develop headaches related to high blood pressure or their doctors may detect high blood pressure during a routine physical exam. Because high blood pressure can cause kidney damage, it is very important to treat it. In fact, treatment of high blood pressure can help slow or even prevent kidney failure. Fluttering or pounding in the chest About 25% of PKD patients have a so-called floppy valve in the heart, and may experience a fluttering or pounding in the chest as well as chest pain. These symptoms almost always disappear on their own but may be the first hint that someone has PKD. How is PKD diagnosed? Ultrasound is the most reliable, inexpensive and non-invasive way to diagnose PKD. If someone at risk for PKD is older than 40 years and has a normal ultrasound of the kidneys, he or she probably does not have PKD. Occasionally, a CT scan (computed tomography scan) and MRI (magnetic resonance imaging) may detect smaller cysts that cannot be found by an ultrasound. MRI is used to measure and monitor volume and growth of kidneys and cysts. In some situations, genetic testing might also be done. This involves a blood test that checks for abnormal genes that cause the disease. Genetic testing is not recommended for everyone. The test is costly, and it also fails to detect PKD in about 15% of people who have it. However, genetic testing can be useful when a person: has an uncertain diagnosis based on imaging tests has a family history of PKD and wants to donate a kidney is younger than 30-years old with a family history of PKD and a negative ultrasound, and is planning to start a family

Liposuction procedure under local anesthesia.

this clip demonstrates the rapid oscillating movements of the eyes in cases of congenital nystagmus.

Over one million Americans have the sexually transmitted virus, HIV, which can lead to the deadly disease known as AIDS.
HIV can be transmitted in the sexual fluids, blood or breast milk of an infected person. HIV prevention therefore involves a wide range of activities including prevention of mother-to-child transmission, needle exchanges and harm reduction for injecting drug users, and precautions for health care workers.
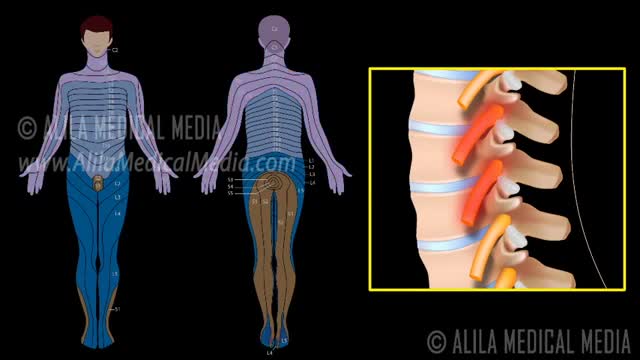
A nerve root block is an injection of local anesthetic (numbing medicine) and steroid injected under X-ray guidance into the area where the nerve exits the spinal column. A nerve root block is usually ordered by your doctor for pain in the arm or leg that follows the path of a single nerve. A nerve root block may be diagnostic (a test to determine the source of your pain) and/or therapeutic (to relieve your pain). If you get a period of sustained pain relief from the injection, the block may be repeated. Sometimes the block is done to help identify whether or not surgery might be helpful and at what level such surgery might be most helpful.

Thai Medical Vacation is the largest medical tours facilitator in Asia. Solutions include Plastic surgery in Thailand,Knee and hip replacements in Thailand,fertility solutions Thailand,cancer therapy in Thailand and stem cell treatments in Thailand, dentistry abroad,and traditional chinese and thai treatments along with orthopedic joint treatments in Thailand

Doctor shares tips on what to expect after a cancer diagnosis
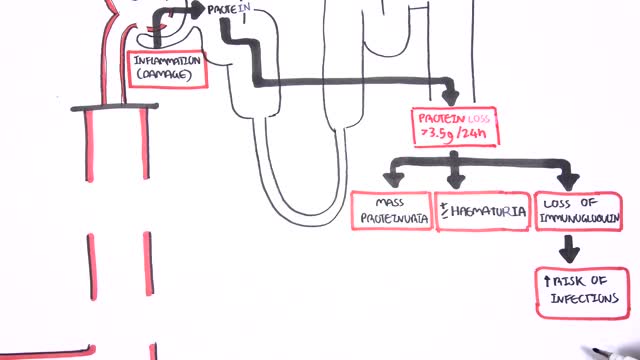
Nephrotic syndrome is a kidney disorder that causes your body to excrete too much protein in your urine. Nephrotic syndrome is usually caused by damage to the clusters of small blood vessels in your kidneys that filter waste and excess water from your blood. Nephrotic syndrome causes swelling (edema), particularly in your feet and ankles, and increases the risk of other health problems. Treatment for nephrotic syndrome includes treating the underlying condition that's causing it and taking medications. Nephrotic syndrome can increase your risk of infections and blood clots. Your doctor may recommend medications and dietary changes to prevent these and other complications of nephrotic syndrome.

Carpal Tunnel Syndrome Ergonomics
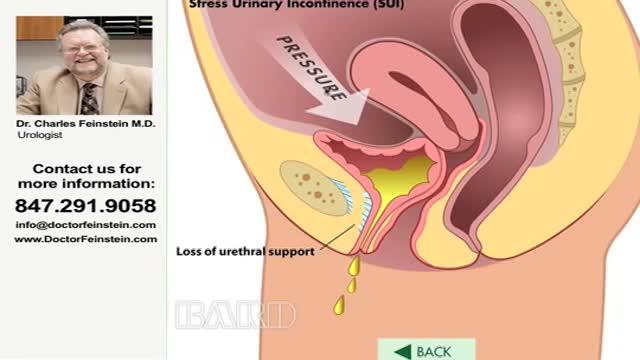
Urinary incontinence — the loss of bladder control — is a common and often embarrassing problem. The severity ranges from occasionally leaking urine when you cough or sneeze to having an urge to urinate that's so sudden and strong you don't get to a toilet in time. If urinary incontinence affects your daily activities, don't hesitate to see your doctor. For most people, simple lifestyle changes or medical treatment can ease discomfort or stop urinary incontinence
Natural Orifice Endoscopic Transgastric Distal Pancreatectomy, A Prospective Randomized Controlled Trial. Natural orifice surgery may represent a paradigm shift in the area of minimally invasive surgery and therapeutic endoscopy. However, studies to date have been limited primarily to small ca...se series with small sample sizes. There has been no large rigorous randomized controlled trial of natural orifice surgery to date. Early work on procedures such as peritoneoscopy, oophorectomy and tubal ligation, while pioneering, have reproduced laparoscopic procedures with minimal morbidity and mortality. In contrast, distal pancreatectomy has a post-operative morbidity of more than 50% even in high volume tertiary care centers. As a highly morbid surgery, the post-operative event rate would allow for a significant difference to be seen in a trial of conventional versus NOTES distal pancreatectomy. We have recently completed a prospective randomized controlled trial of NOTES versus laparoscopic distal pancreatectomy in a swine model which builds on our earlier non-survival work. This video focuses on the endoscopic technique.
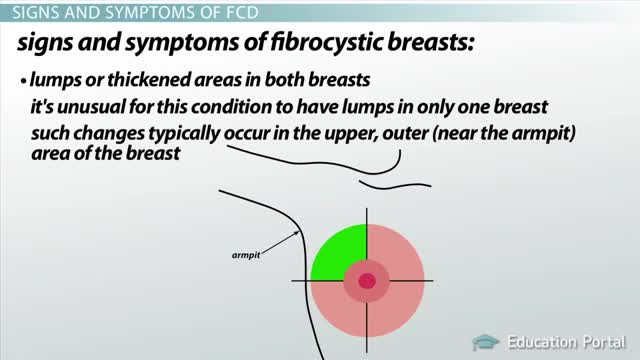
Fibrocystic breasts are composed of tissue that feels lumpy or rope-like in texture. Doctors call this nodular or glandular breast tissue. It's not at all uncommon to have fibrocystic breasts. More than half of women experience fibrocystic breast changes at some point in their lives. In fact, medical professionals have stopped using the term "fibrocystic breast disease" and now simply refer to "fibrocystic breasts" or "fibrocystic breast changes" because having fibrocystic breasts isn't really a disease. Breast changes categorized as fibrocystic are considered normal. Although many women with fibrocystic breasts don't have symptoms, some women experience breast pain, tenderness and lumpiness — especially in the upper, outer area of the breasts. Breast symptoms tend to be most bothersome just before menstruation. Simple self-care measures can usually relieve discomfort associated with fibrocystic breasts.

Detailed examination of the joints is usually not included in the routine medical examination. However, joint related complaints are rather common, and understanding anatomy and physiology of both normal function and pathologic conditions is critically important when evaluating the symptomatic patient. By gaining an appreciation for the basic structures and functioning of the joint, you'll be able to "logic" your way thru the exam, even if you can't remember the eponym attached to each specific test!

Curious about physiotherapy or wanting to know how to properly perform an exercise? Check us out on Social Media! Facebook: https://www.facebook.com/striveptandperformance/ Instagram: https://www.instagram.com/striveptandperf/ Twitter: https://twitter.com/StrivePTandPerf Blog: http://www.strivept.ca/blog
Testosterone treatment in adolescent boys with constitutional delay

Most women have vaginal discharge at many different times throughout their cycle. During ovulation, white and watery discharge is common and accepted as normal. But, discharge after ovulation is widely believed to be a sign of pregnancy.

External cephalic version is a process by which a breech baby can sometimes be turned from buttocks or foot first to head first. External cephalic version (ECV) is a manual procedure that is advocated by national guidelines for breech presentation singleton pregnancy, in order to enable vaginal delivery.

Reverse sural flap for ankle and heel soft tissues reconstruction
The mainstay of treatment is usually medication, talk therapy, or a combination of the two. Increasingly, research suggests these treatments may normalize brain changes associated with depression.

Podalic version is an obstetric procedure wherein the fetus is turned within the womb such that one or both feet present through the cervix during childbirth. It is used most often in cases where the fetus lies transversely or in another abnormal position in the womb.
