- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

#final #fumc #mbbs #medicalstudents #mbbsabroad #doctor #fcps #fcpspart #surgeryeducation #surgeryreview #trainee #exampreparation

In this video, Professor Dan Reinstein performs a bilateral LASIK procedure filmed in real-time to demonstrate the full 8 and-a-half minute procedure from multiple angles. The superior design and experience of the Carl Zeiss Meditec Visumax femtosecond Laser for flap creation is seen, where the patient is only in contact with the device for about 30 seconds with extremely low contract force such that the patient feels effectively nothing, there are no red splodges (subconjunctival haemorages) left behind. From the surgeons' standpoint there is no device that is easier to use or faster for LASIK flap creation. The Carl Zeiss Meditec MEL80 excimer laser portion of the procedure is seamlessly integrated and incorporates all the features that make clinical outcomes so reproducible including the unique cone-for-controlled-atmosphere (CCA) and high efficiency, high sensitivity calibration test which can be performed for each individual patient to compensate for minor changes in energy that occur with excimer laser devices during the course of a day.
For reference to the clinical outcomes for LASIK with the MEL80 in presbyopia using PRESBYOND Laser Blended Vision see:
Reading glasses presbyopia (ageing eyes) only:
LASIK for presbyopia correction in emmetropic patients using aspheric ablation profiles and a micro-monovision protocol with the Carl Zeiss Meditec MEL 80 and VisuMax.
J Refract Surg. 2012 Aug;28(8):531-41. Reinstein DZ, Carp GI, Archer TJ, Gobbe M.
http://www.ncbi.nlm.nih.gov/pubmed/22869232
Short sighted, astigmatism and presbyopia (ageing eyes)
LASIK for Myopic Astigmatism and Presbyopia Using Non-Linear Aspheric Micro-Monovision with the Carl Zeiss Meditec MEL 80 Platform.
J Refract Surg. 2011 Jan;27(1):23-37. Epub 2010 Mar 1.
Reinstein DZ, Archer TJ, Gobbe M.
http://www.ncbi.nlm.nih.gov/pubmed/20205360
Long-sighted, astigmatism and presbyopia (ageing eyes)
LASIK for hyperopic astigmatism and presbyopia using micro-monovision with the Carl Zeiss Meditec MEL80 platform.
J Refract Surg. 2009 Jan;25(1):37-58. Reinstein DZ, Couch DG, Archer TJ.
http://www.ncbi.nlm.nih.gov/pubmed/19244952
For more information about laser eye surgery and PRESBYOND Laser Blended Vision, please contact the London Vision Clinic on 020 7224 1005.

A walk through of an interactive about male to female sex reassignment surgery.

fetal position in womb at 34 weeks fetal position in womb week by week fetal position in womb at 19 weeksUnborn babies toss and turn and hold many different positions within the womb during the gestation period; pregnant women everywhere will attest to the fact that their children always start up the gymnastics at bedtime.

Perineal Protectomy for Rectal Prolapse

When both mucosa and stroma are parts of the suspect lesion, a deep biopsy is needed. The Cervicore is designed to harvest samples from the cervix and vagina with minimal collateral injury to the surrounding tissues. The procedure is easy with minimal discomfort to the patient.

Bleeding from Duodenal Ulcer
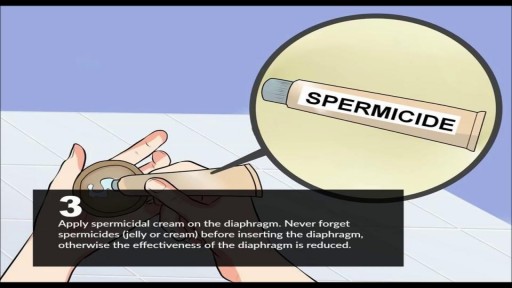
A diaphragm is a shallow, bendable cup that you put inside your vagina. It covers your cervix during sex to prevent pregnancy.
Renal artery stenosis is a narrowing of arteries that carry blood to one or both of the kidneys. Most often seen in older people with atherosclerosis (hardening of the arteries), renal artery stenosis can worsen over time and often leads to hypertension (high blood pressure) and kidney damage.

Watch that video to know if it is safe to have sex during pregnancy or not

Learn about the structural unit of compact bone (the osteon) and it's four basic parts: central canal, lamellae, lacunae, and canaliculi

This is the incredible moment a new-born baby arrived still inside its amniotic sac, completely intact. The tiny infant can be seen moving and stretching still inside the sac, as medics prepare to snip the new born free. The amniotic sac is a thin but durable membrane filled with fluid which helps keep a baby warm and safe from bumps during pregnancy. When it breaks, this is typically referred to as a woman's 'waters breaking' shortly before she gives birth. But in rare cases, less than 1-in-80,000 births, the baby is delivered with the membranes still intact and this is known as a 'caul birth'. Some babies are born with part of the membrane still attached to them, but to be born completely encased in the intact membrane is incredibly rare. Many people still believe the phenomenon to be a good omen for the child's infancy and it is has even been suggested, but not proven, that caul babies will always have a natural affinity for water. The video was taken in Spain on Saturday and captures the rare moment the baby was born with the membrane covering its entire body, just minutes after its twin was delivered normally.

Nosebleeds are common due to the location of the nose on the face, and the large amount of blood vessels in the nose. The most common causes of nosebleeds are drying of the nasal membranes and nose picking (digital trauma), which can be prevented with proper lubrication of the nasal passages and not picking the nose.

Product demonstration video for the Cardinal Health™ Laparoscopic Abdominal Drape (cat. no. 9438)

Train with some of the region’s very best pediatric general surgeons — in a two-year, pediatric surgical fellowship training program at Nemours/Alfred I. duPont Hospital for Children. Our hospital’s Division of Pediatric Surgery is offering this program in affiliation with Sidney Kimmel Medical College at Thomas Jefferson University .
The goal of the fellowship is to give individuals who have completed an accredited general surgery residency advanced knowledge and training in the management and surgical treatment of newborns, infants and children.
Our Fellowship Program
This fellowship will help you prepare for certification by the American Board of Surgery, and is accredited by the Accreditation Council for Graduate Medical Education (ACGME).
The Pediatric Surgery Fellowship aims to:
train a well-rounded, empathetic, safe pediatric surgeon who is confident managing all aspects of the surgical care of children.
steward our fellow in quality improvement projects and methodology, and provide research opportunities.
provide a rigorous didactic curriculum for our fellow utilizing 360 degree feedback.
cultivate opportunities for our fellow to educate residents and students.
encourage our fellow to collaborate across specialties.
develop our fellow’s presentation skills during M&M conferences and multi-disciplinary educational meetings.
The program features the full participation of all nine of the pediatric surgical division’s full-time faculty members. Each of these physicians will contribute greatly to your education. Your training will include operating room and outpatient clinic experience, as well as bedside evaluation of children. You’ll also play a role in the organization of formal teaching conferences, held weekly. Formal rotations will be spent on Pediatric Urology, PICU and Neonatology during the first 12 months. The last year will be spent entirely on the Pediatric Surgical Service.
The majority of your inpatient consultative time will take place at Nemours/Alfred I. duPont Hospital for Children, a freestanding children’s hospital in Wilmington, Del. The hospital:
is nationally ranked by U.S. News & World Report in eight pediatric specialties
recently opened expansion with 260 beds
performs more than 2,800 inpatient and 9,300 outpatient surgical procedures each year in our operating rooms
has an on-site delivery center for newborns with complex congenital anomalies
receives more than 50,000 annual visits in our Emergency Department (ED)
is accredited by The American College of Surgeons as a Level One Pediatric Trauma Center
is accredited by the Commission on Accreditation of Rehabilitation Facilities (CARF)
Visit https://www.nemours.org/educat....ion/gme/fellowships/ to learn more.

A patient suffering from Diabetic gangrene and maneged by "myiasis"

Twin Childbirth Video

Focal seizures (also called partial seizures [citation needed] and localized seizures) are seizures which affect initially only one hemisphere of the brain. [citation needed] The brain is divided into two hemispheres, each consisting of four lobes – the frontal, temporal, parietal and occipital lobes.

The is a time lapse video animation of a complicated ear infection with a ruptured eardrum causing drainage with eventual healing. The video also shows why a period of hearing loss and clogged/muffled ear sensation may occur.

WARNING: Explicit and Educational Surgical Content.
Visage Clinic's Dr. Marc DuPéré - located in Toronto, Ontario, Canada discusses Liposuction (upper bra, back rolls, lower back rolls, love handles & abdomen) and "Tummy Tuck" (Abdominoplasty): Skin excision, muscle repair and umbilicoplasty.
For more info and to book a consultation visit www.VisageClinic.com/cosmetic-....surgery/mommy-makeov or call (416) 929-9800.
