- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Watch that video to know the Serious Side Effects of Using Steroids
Boqueras Causas, Como Se Quitan Las Boqueras, Porque Salen Boqueras En La Boca, Queilitis Angular --- http://queilitis-angular.good-info.co --- Hay Que Actuar Ante Los Primeros Signos De Queilitis Angular. Las Primeras Manifestaciones De Queilitis Angular Suelen Ser Tenues Y Apenas Molestas. Pero No Por Ello Hay Que Ignorarlas, Porque Pueden Derivar En Problemas Mayores. La Queilitis Angular O Lo Que Comúnmente Se Llaman Boqueras, Comienza Por Grietas Minúsculas En Los Extremos De La Boca. También Se Empieza A Sentir Ardor Y Molestias Al Mover Los Labios O Al Abrir La Boca. ¿Qué Sucede Si No Se Atienden De Inmediato Esas Pequeñas Molestias? Difícilmente Se Irán Por Si Solas Sino Que, Por El Contrario, Comenzarán A Agravarse. Las Minúsculas Grietas Se Harán Cada Vez Más Pronunciadas Por El Continuo Movimiento De La Boca. Al Intensificarse Las Grietas Pueden Llegar A Convertirse En Llagas Y A Sangrar. Y Las Infecciones No Tardarán En Aparecer. La Queilitis Angular Puede Ser En Un Primer Momento Molesta Para Quien La Sufre. A Medida Que Avanza, Las Pequeñas Manifestaciones En La Boca Comienzan A Ser Bien Visibles Y Desagradables. Por Lo Que Al Ardor, Picazón Y Dolor, Se Le Suma El Hecho De Querer Ocultar La Afección Ante Los Demás. Cosa Que No Es Fácil De Lograr. A Pesar De Ser Pequeña, La Boca Es Uno De Los Lugares Más Visible Y Observado. Si Hablamos, Comemos, Bebemos, Nuestra Boca Está En Primer Plano. Ante Los Primeros Signos De Queilitis Se Puede Recurrir A Una Crema O Pomada Adecuada, Antiséptica, Antimicótica O Antifúngica. Si Bien Los Extremos De La Boca Deben Permanecer Libres De Saliva O Transpiración, Deben Estar Bien Hidratados. Cualquier Crema Antiséptica Que Se Utilice Debe Ser Libre De Perfumes Y Colorantes Químicos. Debe Detener La Descamación, A La Vez Que Calmar El Picor. El Área Afectada Tendrá Que Permanecer Bien Aseada, Procediendo A Secarla Sin Frotar, Como Para Que No Se Resienta Aún Más La Piel De Los Labios Y Sus Adyacencias. Para Curar La Queilitis Angular No Alcanza Con Los Tópicos Que Se Puedan Utilizar, Por Más Efectivas Que Sean Sus Fórmulas Desde Las Primeras Aplicaciones. Hay Que Llevar A Cabo Una Nutrición Balanceada, Variada Y Suficiente, Con Vitaminas, Minerales Y Oligoelementos. Un Análisis De Laboratorio Podrá Determinar Si Está Haciendo Falta El Aporte De Alguna Vitamina O Mineral. Asimismo, Conviene Evitar Los Lugares Muy Fríos Y/O Húmedos, Así Como Los Espacios Contaminados Por Polvillos O Cualquier Sustancia Irritante Para La Piel. Recomendamos Siempre Actuar Ante Los Primeros Síntomas De Queilitis. Si Se Frena La Dolencia Antes De Que Prospere Y Haga Eclosión, Se Evitará El Sufrimiento Que Puede Implicar Lidiar Contra Lesiones Serias En La Boca. Y Se Evitarán Las Temibles Huellas De Cicatrices Que Pueda Dejar Una Afección Prolongada. ¿Qué Podemos Hacer Ya Mismo? Hoy Existe Un Novedoso Tratamiento, Totalmente Natural Y Muy Simple, Con El Que Se Puede Eliminar La Queilitis Angular O Boqueras En Tan Solo 7 Días (O Menos). Este Revolucionario Sistema Ataca La Verdadera Causa De La Enfermedad Y No Solo Los Síntomas, Asegurando Resultados A Largo Plazo. Si Usted Desea Eliminar Para Siempre Esas Grietas Dolorosas Y La Vergüenza Que Causa Esta Afección, Puede Conocer Este Método De Resultados Comprobados Haciendo Clic En El Siguiente Enlace http://queilitis-angular.good-info.co


Pregnancy occurs when an egg is fertilized by a sperm, grows inside a woman's uterus (womb), and develops into a baby. In humans, this process takes about 264 days from the date of fertilization of the egg, but the obstetrician will date the pregnancy from the first day of the last menstrual period (280 days 40 weeks).

ESCLEROTERAPIA
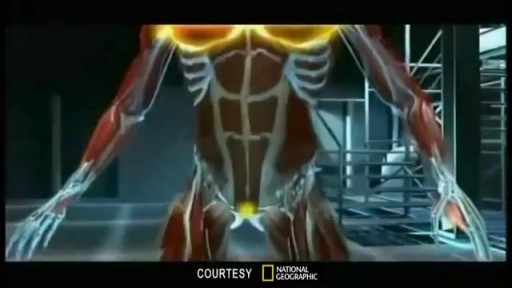
Fibrodysplasia ossificans progressiva (FOP) is a disorder in which muscle tissue and connective tissue such as tendons and ligaments are gradually replaced by bone (ossified), forming bone outside the skeleton (extra-skeletal or heterotopic bone) that constrains movement. This process generally becomes noticeable in early childhood, starting with the neck and shoulders and proceeding down the body and into the limbs. Extra-skeletal bone formation causes progressive loss of mobility as the joints become affected. Inability to fully open the mouth may cause difficulty in speaking and eating. Over time, people with this disorder may experience malnutrition due to their eating problems. They may also have breathing difficulties as a result of extra bone formation around the rib cage that restricts expansion of the lungs.


Celebrity hair stylist Michael DeMarse of Houston, TX shares his experience with us. Michael has been a loyal patient of Dr. Jue for a long time! Call us for a free consultation at (281) 277-9200 or visit https://www.sugarlanddentalspa.com/

Research from Mayo Clinic finds that half of elderly patients who start dialysis after age 75 will die within one year.
Lead study author and a health care delivery scholar with the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Dr. Bjorg Thorsteinsdottir says many elderly patients and their families feel that they have no choice but to start dialysis, with several expressing regret from having initiated therapy.
The findings were presented at the American Society of Nephrology's Kidney Week 2013 in Atlanta.

Demystify knee pain and discover nine of the most common causes of pain in this complex joint. Join Burke Selbst PT as we work through our simple screening for the most common types of problems.
Burke is the founder and clinical director of Focus Physical Therapy in Bend Oregon.
Find him:
https://focusptbend.com
https://facebook.com/focusphysio
Intro Song Credit
Adventures by A Himitsu https://www.youtube.com/channel/UCgFw...
Creative Commons — Attribution 3.0 Unported— CC BY 3.0
http://creativecommons.org/licenses/b...
Music released by Argofox https://youtu.be/8BXNwnxaVQE
Music provided by Audio Library https://youtu.be/MkNeIUgNPQ8

Get my book on fixing injury here:
https://www.amazon.com/Rebuild....ing-Milo-Foundation-
Get my book 'The Squat Bible' here:
https://www.amazon.com/Squat-B....ible-Ultimate-Master
Get my 13-Week Squat Program? https://marketplace.trainheroi....c.com/workout-plan/p
Get olympic weightlifting programming (part 1):
https://marketplace.trainheroi....c.com/workout-plan/p
Get olympic weightlifting programming (part 2): https://marketplace.trainheroi....c.com/workout-plan/p
______________________
Show Sponsors
- TYR: https://www.tyr.com/?gclid=Cjw....KCAjw9qiTBhBbEiwAp-G
- Bandbell: Check out their amazing bars here: https://www.bandbell.com/?utm_source=youtube.com&utm_medium=web&utm_campaign=squatu
______________________
Subscribe to the channel: https://tinyurl.com/y2eq7kpr
Check out the Eleiko products I use here: https://shop.eleiko.com/en-us/?ref=qg8uBQd3JL7S
Recommended products: https://squatuniversity.com/recommended-products/
FitMap: https://www.fitmaptrainer.com/
Support SquatU & join monthly live Q&A: https://www.patreon.com/SquatUniversity
______________________
Connect with SquatUniversity:
Visit the website: http://www.squatuniversity.com
Like the Facebook page: https://www.facebook.com/SquatUniversity
Follow on Twitter: https://twitter.com/squatuniversity
Follow on TikTok: @SquatUniversity
Follow on Instagram: http://instagram.com/squat_university
Listen to the Podcast on: apple iTunes, Overcast, Pocket Casts, Google Play and the Anchor App
Shout out @Muscle and Motion for the amazing anatomy graphics.
______________________

Emory has one of the few heart and vascular centers nationally performing robotic cardiac surgery using the daVinci Surgical System. Emory's robotic surgeons have completed numerous cases and are recognized in Atlanta, the Southeast and across the country for their expertise in cardiac surgery. Some of the cardiac and thoracic conditions treated by Emory cardiac surgeons include mitral valve repair and replacement, atrial septal defect repair, atrial myxoma and thrombi, coronary bypass (LIMA to LAD), mediastinal mass excision, thymectomy, epicardial lead placement and pericardial window.

When a ventral hernia occurs, it usually arises in the abdominal wall where a previous surgical incision was made. In this area the abdominal muscles have weakened; this results in a bulge or a tear. In the same way that an inner tube pushes through a damaged tire, the inner lining of the abdomen pushes through the weakened area of the abdominal wall to form a balloon-like sac. This can allow a loop of intestines or other abdominal contents to push into the sac. If the abdominal contents get stuck within the sac, they can become trapped or “incarcerated.” This could lead to potentially serious problems that might require emergency surgery.

Observation of both jugular veins can provide a reliable indication of the volume and pressure in the right side of the heart since internal jugular veins pulsate in response to phasic changes in right atrial pressure. Proper positioning of the patient to increase the effects of gravity enhances distention of the jugular veins and, therefore, increases the ability to observe venous pulsations.

A video showing how to perform knot tying

Cannula are often introduced into blood vessels in 80% of patients in the hospital for treatment. This can be a daunting experience to patients and stressful to doctors as multiple attempts are used. This may result in introducing spreading MRSA, E Coli & Chlostredium living on your skin into blood and results in Invasive MRSA infection.
Skin is often not adequatly cleaned during subsequent atempts as doctors/nurses do not wait for 1 min after applying cleaning solution on the skin before they puncture your skin.
Multiple punctured sites allow CA-MRSA to enter blood stream resulting in bacteremia and death.
Our mission is to reduce spreading invasive CA-MRSA in the hospitals by developing alternative technique to introduce cannulae.
Medifix was created by doctors with a mission to reduce the threat of spreading antibiotic resustant bacteria to mankind.

A video of appendectomy surgery performed by the laparoscope

A vidoe showing the pronator drift from the USMLE collection
