- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
This video demonstrates how to test for trace amounts of blood in the patients stool. Trace amounts of blood in the stool can be sign of a number of problems, colon cancer being the most worrisome.

At Children's Hospital, Dr. Mary Bedard and the NICU nursing staff save the life of a tiny infant struggling from a serious intestinal infection. ~ Detroit Medical Center
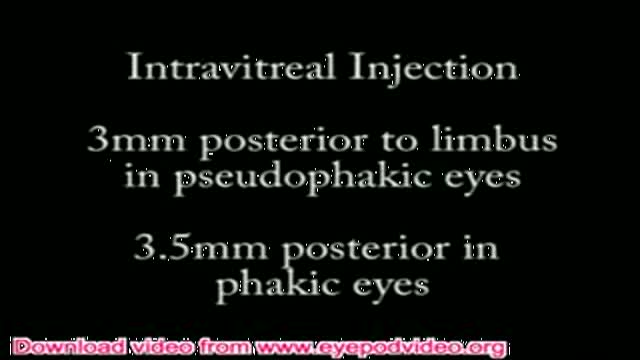
Instructional video explaining intravitreal injection technique used in endophthalmitis (a serious eye infection), macular degeneration, and other eye diseases.

An Echocardiography showing an Acute Pulmonary Embolism

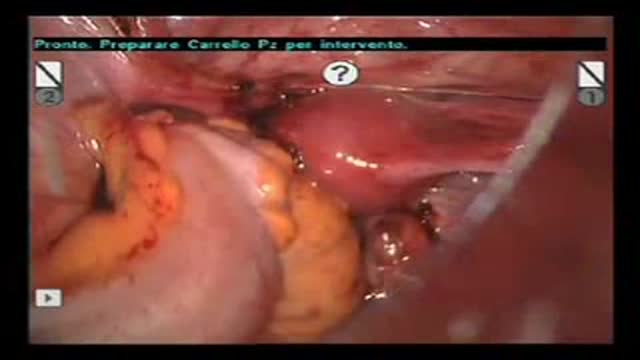
The Digging and Peeling off method is of absolute value to the laparoscopic myomectomy since that can provide time necessary to remove the large and multiple leiomyoma and suture the uterus. Please do not hesitate to contact us if you require any further information or help, it will be a pleasure for mr to assist you. e-mail : eunds1212@yahoo.co.kr homepage : www.eunhospital.co.kr

This 25 second video clip demonstrates the effect of "post-tetanic facilitation" in a patient receiving rocuronium (a neuromuscular blocking agent)under general anesthesia

A plastic surgery video showing Turbinal Reduction and Turbinoplasy of the nose
Robot-Assisted Laparoscopic Rectal Resection for Endometriosis
Causes of declining libido in women

Laparoscopic varicocellectomy Surgery

أ.د/ سمير عبد الغفار في برنامج الصحة و الجمال يتحدث عن الطرق العلاجية المختلفة لعلاج الأورام الليفية في الرحم و خاصة بالطرق التي تتفادى استئصال الرحم.
أ.د/ سمير عبد الغفار هو استشاري العمليات التداخلية بدون جراحة في كلية الطب بجامعة عين شمس
للمزيد من المعلومات عن الأورام الليفية في الرحم:
http://www.Fibroidstoday.com
Associate Professor Dr. Samir Abd Elghaffar spekaing in the famous TV show "Health and Beauty" discussing various non invasive techniques of curing fibroids and leiomyomas stressing on the interventional radiology techniques.
Dr. Samir Abd Elghaffar is the consultant of interventional radiology and non invasive procedures in Ain Shams Faculty of medicine.
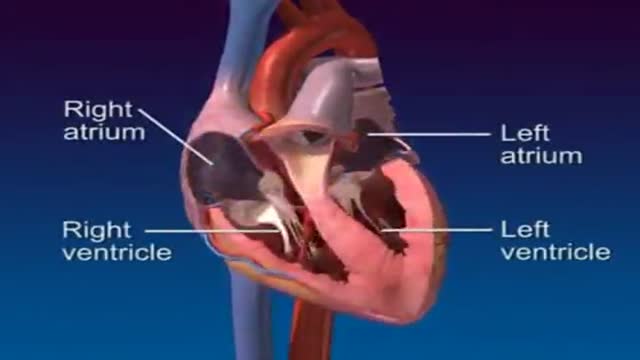
A 3D video clip showing anatomy and physiology of the heart

Mr. Dan underwent 5 suregries in a single go-Both sided hernias+both sided varicocoele and one hydrocoele.Our web site: http://www.desarda.com “Complete cure from groin hernia is now possible with Dr.Desarda's repair technique.......” Mesh is a foreign body, a simple piece of cloth prepared from the synthetic threads. Therefore, its use in inguinal hernia repairs is known to cause all sorts of complications like pain, recurrence, infection etc. We have developed an innovative new technique of inguinal hernia repair without mesh. It uses your own body muscle for repair and gives virtually complete cure from inguinal hernia problem. An undetached strip of the external oblique aponeurosis is stitched on the weak area between the muscle arch and the inguinal ligament to form a new, strong and physiologically dynamic posterior wall that gives protection and prevents re-herniation. Normally patient goes home in a day after surgery and can drive car and go to office in 3-4 days time. This "Dr.Desarda's hernia repair" is now followed in many countries all over the world. We are surprised to see the enquiries from many patients in the developed countries asking for this repair in their country. This is because this operation does not use any foreign body like mesh for repair and therefore there are no complications that are seen in mesh repairs. A visit to Topix or other hernia forums show thousands of posts showing sufferings of many patients due to mesh repairs. But still why surgeons from developed countries are interested in mesh repairs is a big question for us. Please visit our website for more details: http://www.desarda.com or http://herniasurgery.tripod.com Our cell number: +91 9373322178

GYNECOMASTIA IN QATAR video
This clip shows the basic steps of inserting V.T> tubes. This surgery is performed for the treatment of OME resistent to medical TTT.

HD Cataract Surgery Video

Thyroid Exam Physical Exam
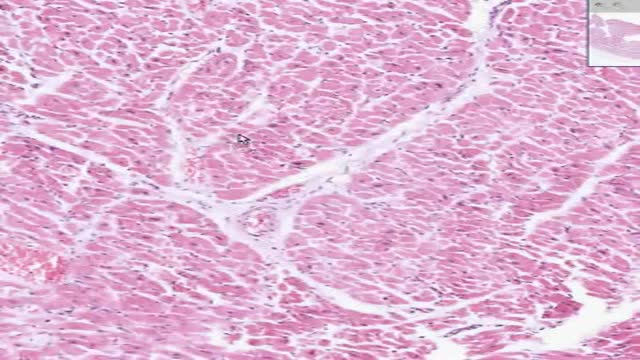
Histology of Heart Endocardium Pericardium Epicardium

Histology of Rectoanal Junction
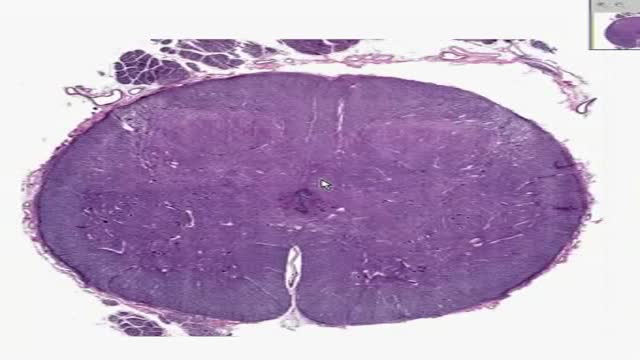
Histology of Spinal Cord
