- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Histology of Rectoanal Junction
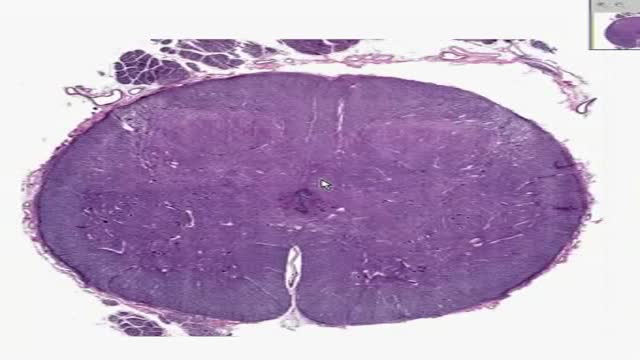
Histology of Spinal Cord

Cricothyrotomy Quick Airway Access
Targeted approach helps patients better manage prostate cancer and inhibit adrogen production.
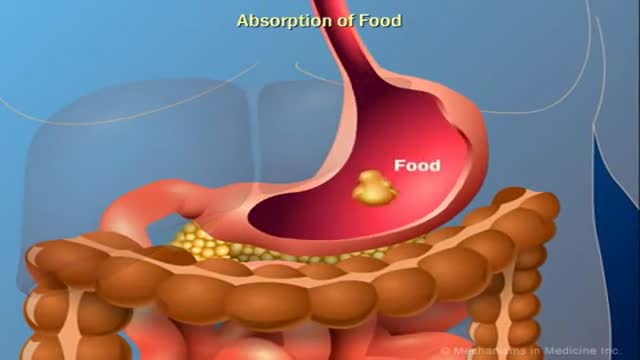
The Role of Insulin in the Human Body

Hiatal Hernia 3D Medical Animation
Women Health Tips: Importance of getting a pap smear, breast exam, and mammogram

Dr Allen’s device provides a new kidney stones treatment that tackles the cause of kidney stone formation which is hidden at the capillary level, read at http://www.finetreatment.co.uk. The unique natural Thermobalancing Therapy does not use harmful medication or shock waves and, of course, surgery. Learn by watching this video about kidney stones cause and how to dissolve kidney stone or kidney stones at home by using Dr Allen’s natural therapeutic device.
http://www.HypothyroidismCure.blog300.com - Hypothyroidism Treatment Natural - Hypothyroidism Recipes Treatment
Let’s Get Something Straight…
* You’re here because you’re serious about overcoming your hypothyroidism…
* You’re here because you’re serious about and taking back your life…
* You know there’s no magic pill to cure your hypothyroidism and never will be…
Hypothyroidism Treatment Natural - Hypothyroidism Recipes Treatment

http://www.landging.com/annulus_pressure_responsive.html
This annulus pressure responsive (APR) animation demonstrates new oil drilling technology.

Please watch and share with your firends and family who smoke
The purpose of an ELISA is to determine if a particular protein is present in a sample and if so, how much. There are two main variations on this method: you can determine how much antibody is in a sample, or you can determine how much protein is bound by an antibody. The distinction is whether you are trying to quantify an antibody or some other protein. In this example, we will use an ELISA to determine how much of a particular antibody is present in an individuals blood.
ELISAs are performed in 96-well plates which permits high throughput results. The bottom of each well is coated with a protein to which will bind the antibody you want to measure. Whole blood is allowed to clot and the cells are centrifuged out to obtain the clear serum with antibodies (called primary antibodies). The serum is incubated in a well, and each well contains a different serum (see figure below). A positive control serum and a negative control serum would be included among the 96 samples being tested.

laparoscopic appendcectomy

Skin Whitening Pills in Pakistan can be bought here at a reasonable price. Glutathione whitening pills gradual and permanent skin whitening results for everyone
FUE (follicular unit extraction) is a minimally invasive method in hair transplantation. Unlike strip harvesting, the traditional technique in which a strip of skin is removed from a donor site and cut into individual units, FUE uses an instrument to remove multiple groups of one to four hairs. The great thing about FUE is that there’s no linear scar. The downside is that a fewer number of hair grafts can be gathered per session.
Myocardial infarction (MI), commonly known as a heart attack, is defined pathologically as the irreversible death of myocardial cells caused by ischemia. Clinically, MI is a syndrome that can be recognized by a set of symptoms, chest pain being the hallmark of these symptoms in most cases, supported by biochemical laboratory changes, electrocardiographic (ECG) changes, or findings on imaging modalities able to detect myocardial injury and necrosis. According to the third universal definition of MI, implemented by a joint task force from the European Society of Cardiology (ESC), American College of Cardiology (ACC) Foundation, American Heart Association (AHA), and the World Heart Federation (WHF), MI is diagnosed when either of the following two criteria are met
Thalassemia is an inherited blood disorder characterized by less hemoglobin and fewer red blood cells in your body than normal. Several types of thalassemia exist, including alpha-thalassemia, beta-thalassemia intermedia, Cooley's anemia and Mediterranean anemia. Hemoglobin is the substance in your red blood cells that allows them to carry oxygen. The low hemoglobin and fewer red blood cells of thalassemia may cause anemia, leaving you fatigued. If you have mild thalassemia, you may not need treatment. But, if you have a more severe form of thalassemia, you may need regular blood transfusions. You can also take steps on your own to cope with fatigue, such as choosing a healthy diet and exercising regularly.
The virus was first discovered in 1964 when Sir Michael Anthony Epstein and Ms. Yvonne Barr found it in a Burkitt lymphoma cell line. In 1968, the virus was linked to the disease infectious mononucleosis. Infection with Epstein-Barr virus (EBV) is common and usually occurs in childhood or early adulthood. EBV is the cause of infectious mononucleosis (also termed "mono"), an illness associated with fever, sore throat, swollen lymph nodes in the neck, and sometimes an enlarged spleen. It is also known as human herpes virus 4. Although EBV can cause mononucleosis, not everyone infected with the virus will get mononucleosis. Less commonly, EBV can cause more serious disease. Symptoms caused by EBV are usually mild and self-limited, but the virus persists in the body for life. It can be reactivated quietly without causing symptoms and may contaminate saliva. Thus, otherwise healthy people can spread the virus to uninfected people through kissing or sharing
Cytomegalovirus (CMV) is a common virus that can infect almost anyone. Most people don't know they have CMV because it rarely causes symptoms. However, if you're pregnant or have a weakened immune system, CMV is cause for concern. Once infected with CMV, your body retains the virus for life. However, CMV usually remains dormant if you're healthy. CMV spreads from person to person through body fluids, such as blood, saliva, urine, semen and breast milk. CMV spread through breast milk usually doesn't make the baby sick. However, if you are pregnant and develop an active infection, you can pass the virus to your baby.
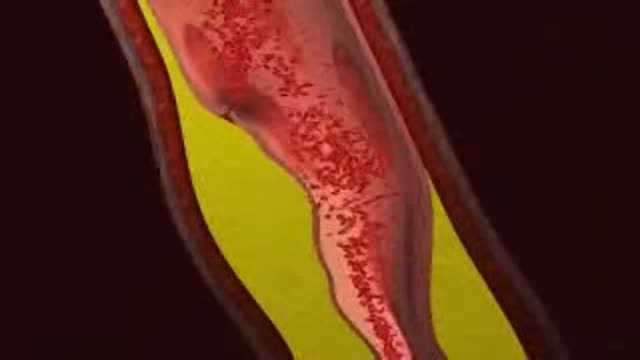
Deep vein thrombosis (DVT) occurs when a blood clot (thrombus) forms in one or more of the deep veins in your body, usually in your legs. Deep vein thrombosis can cause leg pain or swelling, but may occur without any symptoms. Deep vein thrombosis can develop if you have certain medical conditions that affect how your blood clots. Deep vein thrombosis can also happen if you don't move for a long time, such as after surgery, following an accident, or when you are confined to a hospital or nursing home bed. Deep vein thrombosis is a serious condition because blood clots in your veins can break loose, travel through your bloodstream and lodge in your lungs, blocking blood flow (pulmonary embolism).
