- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
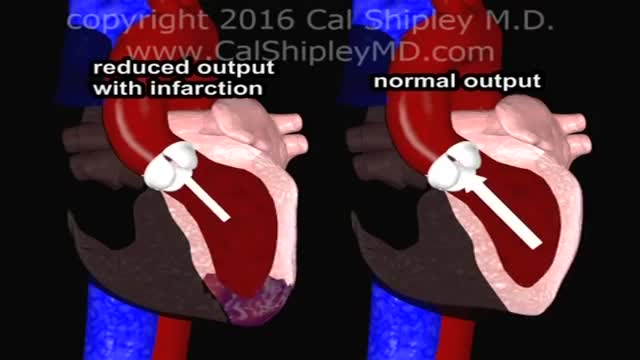
Cardiogenic shock is a condition in which your heart suddenly can't pump enough blood to meet your body's needs. The condition is most often caused by a severe heart attack. Cardiogenic shock is rare, but it's often fatal if not treated immediately. If treated immediately, about half the people who develop the condition survive.
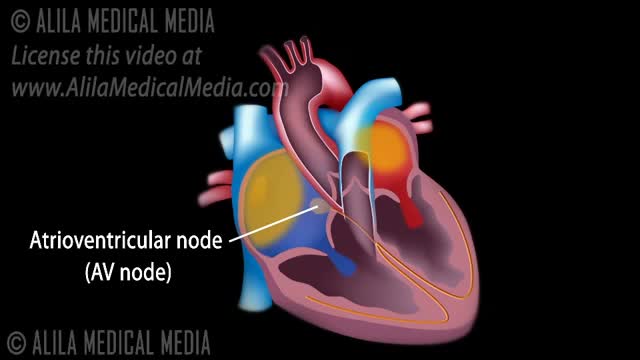
The normal electrical conduction in the heart allows the impulse that is generated by the sinoatrial node (SA node) of the heart to be propagated to (and stimulate) the cardiac muscle (myocardium). The myocardium contracts after stimulation.

Tests. This test tracks electrical signals from the brain. There are a number of blood tests that may be recommended as part of your epilepsy diagnosis and treatment. A positron emission tomography (PET) scan may be used to locate the part of the brain that is causing seizures.
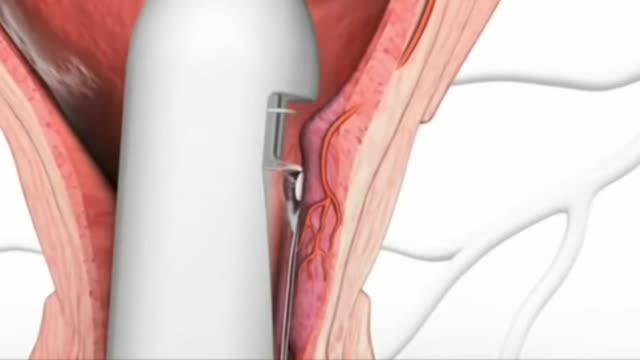
Stapling is used to treat prolapsed hemorrhoids. A surgical staple fixes the prolapsed hemorrhoid back into place inside your rectum and cuts off the blood supply so that the tissue will shrink and be reabsorbed. Stapling recovery takes less time and is less painful than recovery from a hemorrhoidectomy.

atrial septal defect (ASD) is a hole in the wall between the two upper chambers of your heart (atria). The condition is present from birth (congenital). Small atrial septal defects may close on their own during infancy or early childhood. Large and long-standing atrial septal defects can damage your heart and lungs. Small defects may never cause a problem and may be found incidentally. An adult who has had an undetected atrial septal defect for decades may have a shortened life span from heart failure or high blood pressure that affects the arteries in the lungs (pulmonary hypertension). Surgery may be necessary to repair atrial septal defects to prevent complications
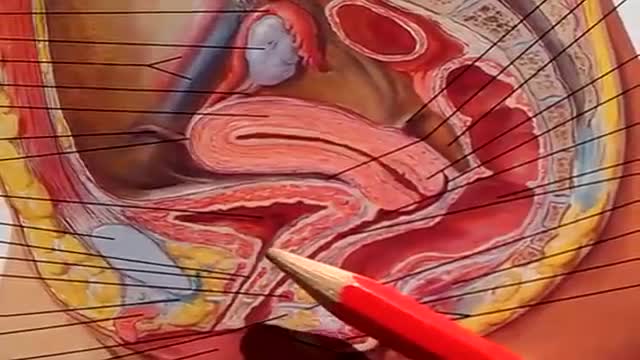
The urinary bladder is a hollow muscular organ that collects urine from the kidneys before disposal by urination. A hollow muscular, and distensible (or elastic) organ, the bladder sits on the pelvic floor. Urine enters the bladder via the ureters and exits via the urethra.

http://tipps-gegen-cellulite.good-info.co --- Was Tun Gegen Cellulite, Ernährung Bei Cellulite, Anti Cellulite übungen, Cellulite Sport. Cellulite: Das Karma Aller Frauen. Cellulite betrifft mehr als 90% der Frauen nach der Pubertät. Wir finden unterschiedlichen Cellulite Graden und die häufigste ist als Orangenhaut bekannt. Wir verwenden den Begriff “Cellulite”, um die Fettablagerungen unter der Haut zu beschreiben. Diese Fett verursacht die Grübchen der Hüften, Oberschenkel, Gesäß und Bauch. Diese Bedingung betrifft fast ausschließlich Frauen und tritt selten bei Männern. Im Gegensatz zu dem verbreiteten Glaube, Cellulite hat nichts mit Übergewicht zu tun. Cellulite wird in beiden übergewichte und dünne Menschen gefunden. Der Markt bietet verschiedene Möglichkeiten, um Cellulite zu bekämpfen, aber in den meisten Fällen sind diese Methoden nicht wirksam. Sowohl Cremen als auch Massage oder andere Art von Cellulite Entfernung geben keine befriedigenden Ergebnisse. Es gibt verschiedene Faktoren, die Cellulite verursachen. Einer der wichtigsten ist die hormonelle Faktor. Die hormonelle Veränderungen während der Pubertät, Schwangerschaft, Wechseljahre oder wenn Sie mit Antibabypillen beginnen. Die Hormone regulieren die Veränderungen im Blutfluss, Lymphdrainage, Fett-und Bindegewebe, die die Bildung von Cellulite verursachen. Mangel an Bewegung ist auch eine sehr wichtige Ursache. Der Bewegungsmangel verursacht nicht nur das Erscheinungsbild der Cellulite, sondern auch verschlechtert ihr Aussehen im Laufe der Zeit. Sie können Ihre Cellulite ab heute mit “Schluss Mit Cellulite“ reduzieren. Klicken Sie hier, um mehr zu erfahren http://tipps-gegen-cellulite.good-info.co

The lumps may be hard or rubbery and can appear as a single breast lump that may be large or small. Fibrocystic changes also can appear as thickening of the breast tissue. Fibrocystic changes can occur in one or both breasts and are the most common cause of benign breast lumps in women age 35 to 50.

Controlled studies on treatment of catscratch disease (CSD) are lacking. Thus, treatment recommendations are based on case reports, reviews, a single controlled trial, and anecdotal data. Practice guidelines for the diagnosis and management of skin and soft-tissue infections, including CSD, have been established.Oct 19, 2016

The heart is the body's engine room, responsible for pumping life-sustaining blood via a 60,000-mile-long (97,000-kilometer-long) network of vessels. The organ works ceaselessly, beating 100,000 times a day, 40 million times a year—in total clocking up three billion heartbeats over an average lifetime. It keeps the body freshly supplied with oxygen and nutrients, while clearing away harmful waste matter.
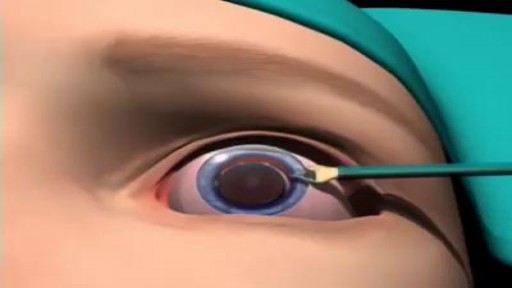
Most cataracts are associated with the aging process and are common among older Americans. In fact, according to the National Eye Institute (NEI), 68.3 percent of Americans 80 and older had cataracts in 2010. And the prevalence of cataracts in the U.S. is expected to grow significantly in the years ahead, due in part to the aging of the population. In 2010, roughly 24.4 million Americans had cataracts, and that number is projected to grow to 50.2 million by the year 2050, according to NEI.
Recovery can take 4 to 6 months, depending on the size of the tear and other factors. You may have to wear a sling for 4 to 6 weeks after surgery. Pain is usually managed with medicines. Physical therapy can help you regain the motion and strength of your shoulder.

Ventral Hernia Repair

Cosmetic Eye and Eyelid Surgery

irregular, curved toenails. footwear that places a lot of pressure on the big toes, such as socks and stockings that are too tight or shoes that are too tight, narrow, or flat for your feet. toenail injury, including stubbing your toe, dropping something heavy on your foot, or kicking a ball repeatedly. poor posture. How can ingrowing toenails be prevented? Cut your nails straight across; do not cut them too short or too low at the sides. ... Keep your feet clean and dry. ... Avoid tight shoes and use cotton socks rather than synthetic. If you have diabetes, you should take extra care when cutting your nails:
Watch that video to know if oral sex can cause cancer
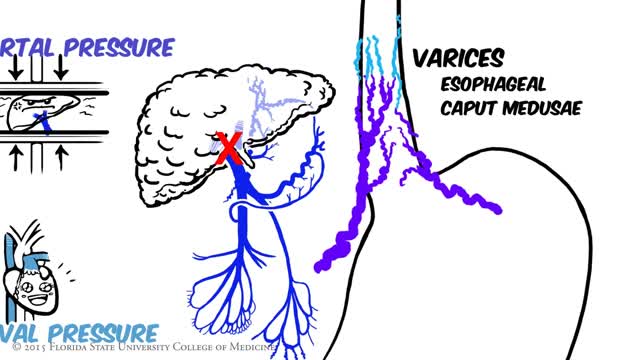
Portal hypertension is an increase in the blood pressure within a system of veins called the portal venous system. Veins coming from the stomach, intestine, spleen, and pancreas merge into the portal vein, which then branches into smaller vessels and travels through the liver.

Although the Apgar score was developed in 1952 by an anesthesiologist named Virginia Apgar, you also might hear it referred to as an acronym for: Appearance, Pulse, Grimace, Activity, and Respiration. The Apgar test is usually given to a baby twice: once at 1 minute after birth, and again at 5 minutes after birth.
Nephritis and Nephrotic Syndrome
Major signs and symptoms include enlargement of the liver and spleen (hepatosplenomegaly), a low number of red blood cells (anemia), easy bruising caused by a decrease in blood platelets (thrombocytopenia), lung disease, and bone abnormalities such as bone pain, fractures, and arthritis.
