- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

basic subcutaneous (SQ) injection techniques

Motor examination of Lower Limb from the USMLE collection
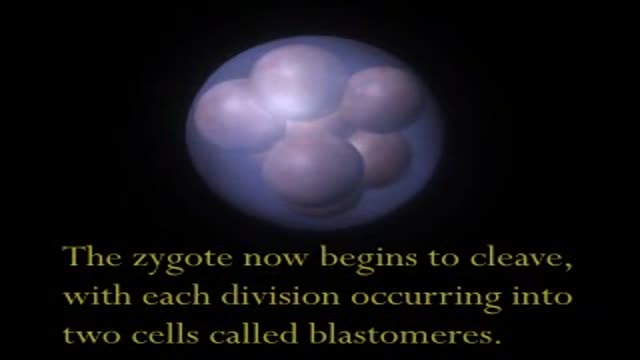
This video shows the process of development and growth of the fetus intrauterine.

The real end for all kinds of migraine was done. You can read all about this video in my web site: www.alisultaneh.8m.com or www.migrainesurgery.4t.com

Removal of pregnancy within the fallopain tube using laparoscopic keyhole surgery. A segment of the tube together with the pregnancy within is removed video.
On screening colonoscopy, this abnormality was encountered in the cecum. This round worm is Ascaris Lumbricoides, one of the most common human parasites in the world. When ingested, the durable Ascaris eggs hatch in the small intestine releasing larva that migrate through the intestinal wall, and t...ravel both hematogenously and lymphatically to the heart and lungs. Over the next several days, the larva mature in the alveoli, then migrate up the trachea to be swallowed back into the gastrointestinal tract. These larva will then mature in the small bowel; adults couples will succeed in producing an extraordinary number of eggs, over 200,000 ova per day. The adults live one to two years. The majority of Ascaris infections are as in this example asymptomatic. Symptoms are a consequence of either the immunologic hypersensitivity of the host to the worm as in the pulmonary stage referred as Loffler's syndrome or to mechanical obstruction of lumen by the worm. Heavy worm burden can result in intestinal obstruction and migrating worms can cause pancreatitis and/or cholangitis when involving the pancreatobiliary tree. Multiple medical therapies are approved for its treatment including mebendazole. Epidemiologically, infections are most common in areas of lower socio-economic conditions. This man manages a pig farm in China that is used to test pharmaceutical agents. From an endoscopic standpoint it is noteworthy that the worms do not like light and will move away fro the attention it is receiving. In this example, the endoscopist was too slow to snare his prey which succeeded in escaping temporarily into the cooler and darker confines of the small bowel out of reach of the endoscope but not from the soon to be consumed anti-helminthic therapy.
Lichtenstein mesh repair of hernia

Surgical technique: A 3cm skin incision under spinal or general anesthesia, depending on the patients’ preference, starts half way the line between the superior anterior iliac spine towards the midline in a 30° angle to the pubic tubercle. Scarpa’s fascia is opened as well as the external obliq...ue aponeurosis. By using this skin line incision the internal ring will be immediately visualized. Although it is important to look for both direct and indirect hernias evaluating the groin, we do not taper the cord and directly evaluate the ring for indirect hernias. In case of an indirect hernia the sac is reduced or resected according to the preference of the surgeon and the preperitoneal space is entered bluntly through the dilated internal ring. In case of a direct hernia the approach slightly differs. One could prefer to open the transversalis fascia through the internal ring over a few centimeters or you can open the fascia more medially, at the site of the direct hernia. As primary point of concern the epigastric vessels should be identified and retracted softly upwards. Then a gauze can be introduced into the preperitoneal space and by doing so most of the space needed medially will be created. Then one can already palpate Cooper’s ligament and the pubic bone. Laterally to the internal ring more digital dissection is needed to create just the appropriate space for the mesh. By placing the mesh it is important not to introduce the mesh too medially. Laterally of the internal ring an adequate overlap of the mesh is necessary, especially in indirect hernias. No splitting of the mesh seems necessary. The patient will be asked to strain and push on the ring to control its place and to check adequate spreading of the mesh to cover the whole myopectineum of Fruchaud. One single stitch of vicryl 3/0 is placed taking both the fascia transversalis and the mesh.

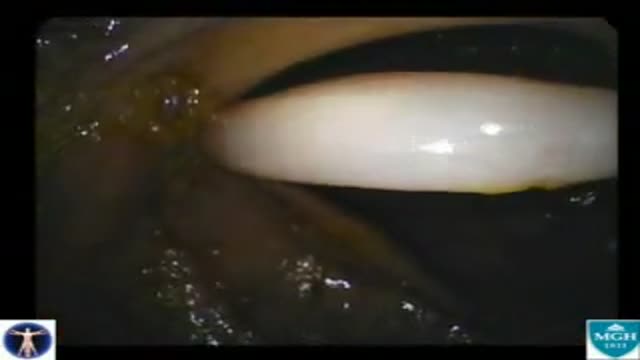
Challenges of cataract surgery in the eye with a history of radial keratotomy include IOL power calculation, protection of the cornea and aviodance of capsular complications.

Descemet’s stripping automated endothelial keratoplasty (DSAEK) avoids a full-thickness corneal procedure and provides rapid visual rehabilitation. Successful graft positioning while minimizing intraoperative donor endothelial trauma may determine long-term graft survival. Previously described t...echniques for graft insertion may be problematic in some patients with intraoperative floppy iris syndrome (IFIS), anatomically shallow or unstable anterior chambers, or intraoperative increased posterior pressure. This video displays alternative method called the suture drag technique, which may facilitate lamellar endothelial graft insertion under these special circumstances.

Stephen has sharing his experience with the others.
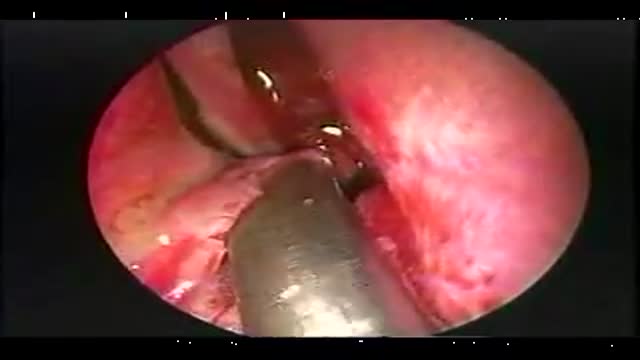
The endoscopic resection of a sharp bony nasal septal spur video

This video demonstrates the approach to a large base of tongue tumor, which was invading the ramus of the mandible. The procedure, named after Dr. Trotter, is really a median labiomandibuloglossotomy. In this case this poorly differentiated tumor was resected along with a portion of the floor of mouth. The entire area was reconstructed with a pectoralis major myocutaneous flap.

Sprains and Strains

Baby CPR

Re-educating the legs to walk again is the ultimate goal of this therapy for those who have suffered a stroke. ~ Detroit Medical Center

DMC Plastic Surgeon Doctor Bruce Chau uses minimally invasive surgery called Liposelection to ultrasonically "melt" fat and remove it, resulting in smoother, younger-looking skin and body. Watch as one patient feels transformed through a procedure to revitalize her breasts and her outlook. ~ Detroit Medical Center

Hallux Valgus Pedis surgery

After a bad fall, a patient suffering from spinal fusion seeks help from a DMC Neurosurgery specialist.
~ Detroit Medical Center
In this video, Dr. Joe Bresee, with CDC's Influenza Division, describes the symptoms of H1N1 (swine flu) and warning signs to look for that indicate the need for urgent medical attention.
