- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
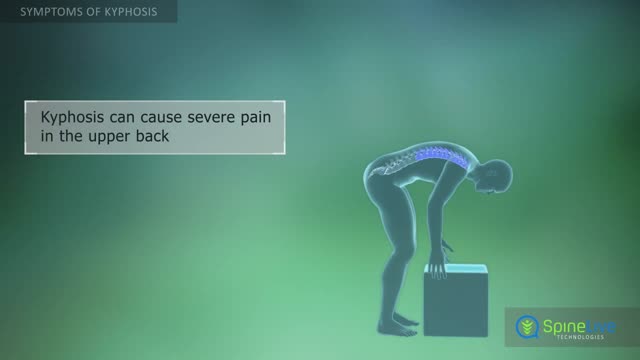
Kyphosis, also known as a round back or hunchback, is a condition in which the spine in the upper back has an excessive curvature. The upper back, or thoracic region of the spine, is supposed to have a slight natural curve.
The usual reason given for people getting fat is that they eat too much and/or exercise too little. That reflects one of the basic laws of thermodynamics—I forget which one. The amount of energy you put into a system minus the energy you take out has to be stored somewhere i.e. FAT! This formulation—true though it is—does not entirely explain obesity since some people seem to eat more than fat people and exercise no more than these same fat people, and yet they are not fat! Chalking this fact up to the general perversity of the universe is not sufficient explanation. Other factors must come into play. I mention below some of the ideas thoughtful people have proposed to explain why fat people become fat:

Direct Laryngoscopy: MICU Fellows Airway Course

The lungs and respiratory system allow oxygen in the air to be taken into the body, while also enabling the body to get rid of carbon dioxide in the air breathed out. Respiration is the term for the exchange of oxygen from the environment for carbon dioxide from the body's cells.

Migraine headaches are recurrent throbbing or pulsatile headaches often associated with a prodrome, nausea, vomiting, photophobia, and phonophobia. When they occur, the prodromes are characterized by visual scintillations, scotomas, dizziness, or tinnitus
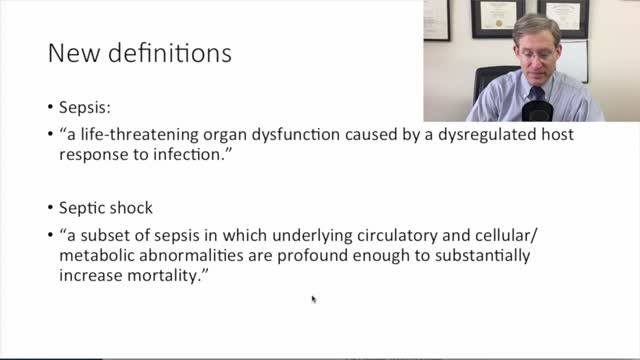
new sepsis definitions
Learn about Bicuspid Aortic Valves in this presentation. Bicuspid Aortic Valves are present in about 2% of the population and are the most common congenital disorder. Find out more about a Bicuspid Aortic Valve by visiting the following link:

Lithium, a mood stabilizer used in bipolar disorder, has a narrow therapeutic index (small difference between therapeutic and toxic levels}. This patient's gradual onset of neurologic symptoms (slurred speech, confusion, tremors, and ataxia) is consistent with chronic lithium toxicity. Therapeutic lithium levels are 0.8- 1.2 mEq/L. Serum lithium levels >1.5 mEq/L confirm toxicity, and levels ;::2 .5 mEq/L require emergency management.
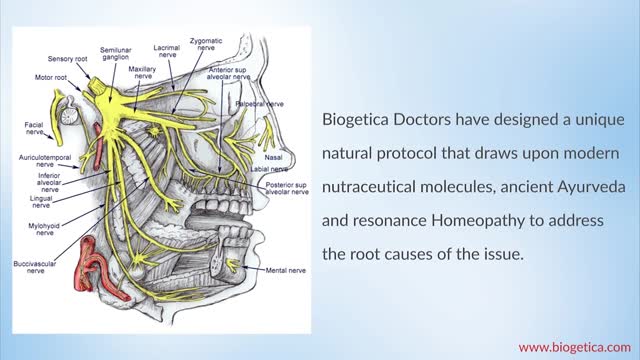
You may initially experience short, mild attacks. But trigeminal neuralgia can progress and cause longer, more-frequent bouts of searing pain. Trigeminal neuralgia affects women more often than men, and it's more likely to occur in people who are older than 50.
Meet Toby, the baby who was born premature at 24 weeks. He may be small, but he's definitely a fighter! Share his story

Duct tape is one home remedy. Put a small strip over the wart and leave it on for six days. Then, remove the tape, soak the wart in water, and then gently debride it with a pumice stone or emory board. Repeat the process many times until the wart is gone.

In a normal hip, the ball at the upper end of the thighbone (femur) fits firmly into the socket, which is part of the large pelvis bone. In babies and children with developmental dysplasia (dislocation) of the hip (DDH), the hip joint has not formed normally.
Angina results from a reduction in the oxygen supply/demand ratio. Therefore, in order to alleviate the pain, it is necessary to improve this ratio. This can be done either by increasing blood flow (which increases oxygen delivery or supply), or by decreasing oxygen demand (i.e., by decreasing myocardial oxygen consumption).
Diagnosis of HIV infection in infants is aided by HIV culture or DNA/RNA polymerase chain reaction (PCR); positive results are confirmed by repeating the test. In suspected cases, HIV testing should occur in the newborn period (ie, before the infant is 48 h old), at age 1-2 months, and again at age 3-6 months.
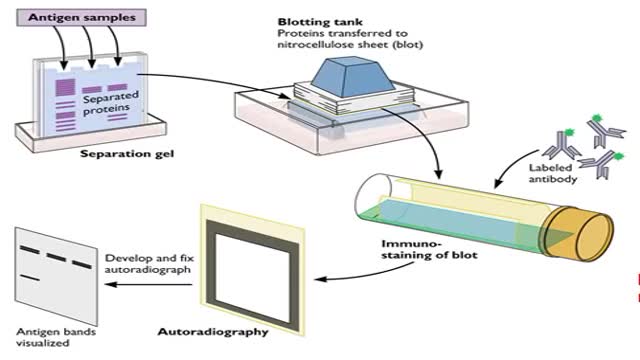
The window period is the time from infection until a test can detect any change. The average window period with HIV-1 antibody tests is 25 days for subtype B. Antigen testing cuts the window period to approximately 16 days and nucleic acid testing (NAT) further reduces this period to 12 days.[2] Performance of medical tests is often described in terms of: sensitivity: The percentage of the results that will be positive when HIV is present specificity: The percentage of the results that will be negative when HIV is not present. All diagnostic tests have limitations, and sometimes their use may produce erroneous or questionable results. False positive: The test incorrectly indicates that HIV is present in a non-infected person. False negative: The test incorrectly indicates that HIV is absent in an infected person.
Your kidneys are two bean-shaped organs that lie just below your rib cage, on each side of your spine. They remove waste from your body, level out your blood pressure, and keep your bones strong. They also ensure that you have the right amount of chemicals, like potassium and sodium (salt), in your blood. Finally, they make the hormone that causes your body to create red blood cells.
Stem Cell Injection Treatment - Stem Cell Therapy
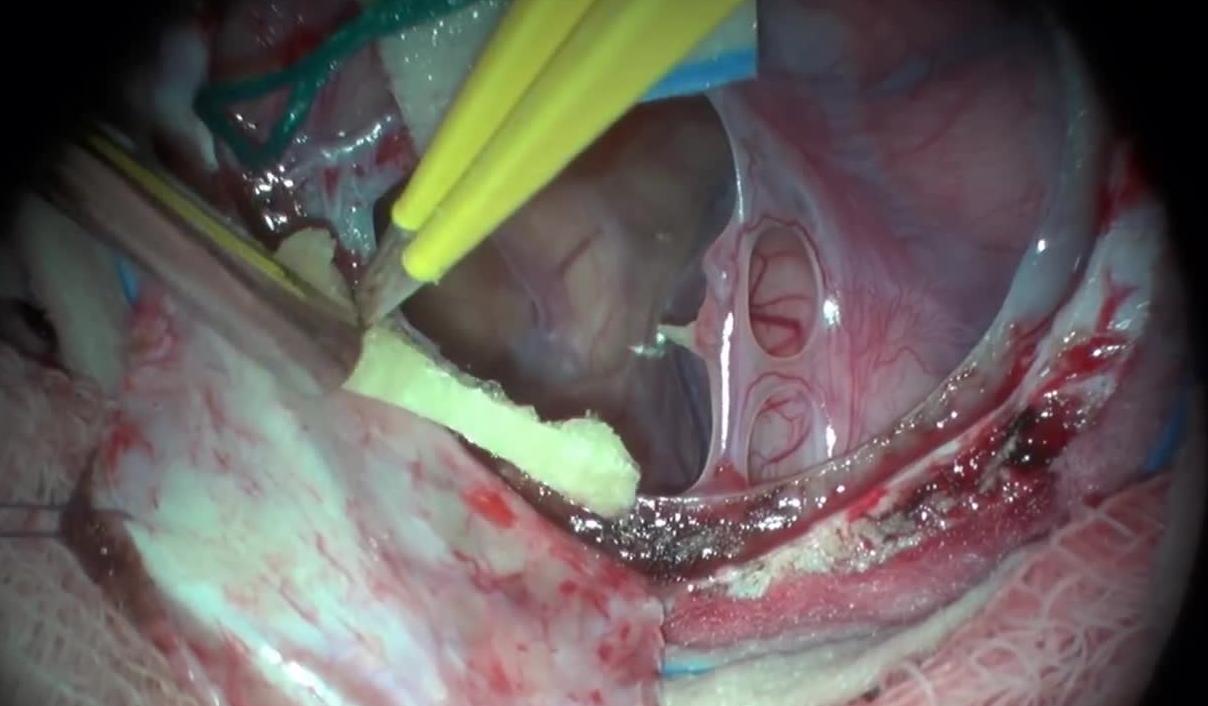
Fenestration of Middle Cranial Fossa Arachnoid Cyst with Accompanying Subdural Hygrom

Dermatomyositis (dur-muh-toe-my-uh-SY-tis) is an uncommon inflammatory disease marked by muscle weakness and a distinctive skin rash. Dermatomyositis affects adults and children alike. In adults, dermatomyositis usually occurs from the late 40s to early 60s. In children, the disease most often appears between 5 and 15 years of age. Dermatomyositis affects more females than males. There's no cure for dermatomyositis, but periods of remission — when symptoms improve spontaneously — may occur. Treatment can clear the skin rash and help you regain muscle strength and function. Symptoms ShareTweet June 17, 2014 References Products and Services Newsletter: Mayo Clinic Health Letter See also Dysphagia Electromyography Fatigue MRI Muscle pain Peptic ulcer Prednisone risks, benefits Show more Advertisement Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission. Advertising & Sponsorship PolicyOpportunitiesAd Choices Mayo Clinic Store Check out these best-sellers and special offers on books and newsletters from Mayo Clinic. NEW! – The Mayo Clinic Diet, Second Edition Treatment Strategies for Arthritis Mayo Clinic on Better Hearing and Balance Keeping your bones healthy and strong The Mayo Clinic Diet Online
A short lecture on albuterol for self-study or review.
