- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

This video was taken 4 days after the surgery. This Patient had a facial rejuvenation procedure performed by Dr. Handal. He was exceptionally pleased with the results. Contact us for a consultation on how our team can help you to look better, (561) 912-9888. https://www.handalplasticsurgery.com

seroma 3 years after surgery

CARDIAC TAMPONADE!!! The surgeon in this video is performing a pericardiotomy in a 30-year-old man that presented to ER after a motor vehicle crash....

Watch that video of a Knife Stabbed Inside Chest Removing Surgery
Watch that video to know How to Have White Thick Sperm
Watch that video of Terrible Horrifying Creatures Found Living Inside a Human Body
Protopic Vitiligo, Weiße Flecken Am Rücken, Pigmentflecken Im Gesicht Entfernen, Flecken Haut--- http://vitiligo-heilung.info-pro.co --- Weiße Flecken auf der Haut: Vitiligo, Die Entwicklung weißer Flecken auf der Haut ist ist ein Symptom einer Hautstörung, die Vitiligo genannt, im deutschen Sprachgebrauch aber auch häufig als "Weißfleckenkrankheit" bezeichnet wird. Man bringt den Zustand mit der Zerstörung oder Fuktionsstörung der Hautzellen in Verbindung, die für die Herstelleung des Hautpigmentes (Melanin) zuständig sind, welches dem Menschen seine Hautfarbe verleiht. Meistens entwickeln sich die Flecken dabei an Stellen, die oft der Sonne ausgesetzt sind, also z.B. die Hände, Arme, Füße, Beine und das Gesicht. Bisweilen treten die Flecken aber auch in den Achselhöhlen, im Genitalbereich und um den Bauchnabel herum auf. Von Vitiligo betroffene erleben häufig auch ein vorzeitiges Ergrauen der Haare. Es wird geschätzt, dass mindestens 1 % der Bevölkerung der Vereinigten Staaten an Vitiligo leidet; in Europe sind die Zahlen ähnlich. Weltweit leiden gegenwärtig mehr als 100 Millionen Menschen an der Hauterkrankung. Die Ursache von Vitiligo Die genaue Ursache der Erkrankung ist noch immer unbekannt. Eine der populärsten Theorien ist jedoch, dass es sich bei Vitiligo um eine Autoimmunstörung handelt. Sie veranlasst das Immunsystem, die Melanozyten (die Hautpigmente produzierenden Hautzellen) anzugreifen. In der Tat haben Menschen, die an einer anderen Autoimmunstörung, wie adrenocorticaler Unterfunktion or Schilddrüsenüberfunktion leiden, ein weitaus höheres Risiko, auch an Vitiligo zu erkranken. Manche Mediziner sind auch der Auffassung, dass Sonnenbrände, emotionaler Stress und bestimte Medikamente die weißen hautflecken hervorrufen könnten. Es wird außerdem geglaubt, dass Vitiligo is also believed eine genetisch vererbte Erkrankung darstellt. Behandlungsoptionen für Vitiligo Für Vitiligo gibt es unterschiedliche Behandlungsmöglichkeiten. Allerdings sind sie allesamt praktisch wirkungslos und beinhalten dazu noch das Risiko, ernsthafte Nebenwirkungen hervorzurufen. Krankenversicherer übernehmen zudem die vollen Behandlungskosten. Das allein macht eine Vitiligo-Behandlung bereits zu teuer für die meisten Patienten, denn es sind üblichwerweise zwei bis drei Besuche wöchentlich in ener Spezialklinik nötig. Ein Paradebeispiel für eine solche Behandlung ist die sogenannte PUVA-Therapie, die ausgesprochen häufig eingesetzt wird. "Gratis-Präsentation enthüllt einen ziemlich ungewöhnlichen Tipp zur Beseitigung von Vitiligo für alle Zeiten und in nur 45-60 Tagen - Garantiert!" http://vitiligo-heilung.info-pro.co Erfahren Sie mehr darüber, indem Sie diese Webseite besuchen: http://vitiligo-heilung.info-pro.co

Watch that video to know the Causes of Pain During Intercourse

Third stage nasal econstuction: Nasolabial flap thinning, caudal septoplasty
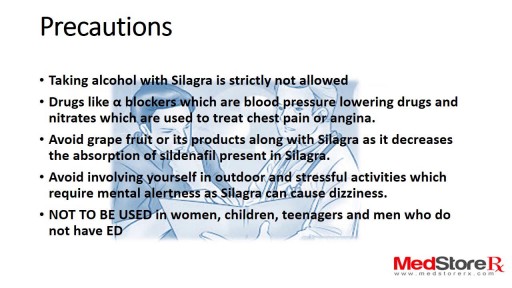
Silagra For Mens ED, medicine approved by FDA, and for more information kindly visit to http://www.medstorerx.com/silagra.aspx

During a surgical procedure to set a fracture, the bone fragments are first repositioned (reduced) into their normal alignment. They are held together with special implants, such as plates, screws, nails and wires.

The cardiovascular system is a closed system if the heart and blood vessels. The heart pumps blood through a closed system of blood vessels. Blood vessels allow blood to circulate to all parts of the body. Arteries usually colored red because oxygen rich, carry blood away from the heart to capillaries within the tissues. Veins usually colored blue because oxygen poor, carry blood to the heart from the capillaries.


Effect of Smoking 30 PACKS of Cigarettes on Your Lungs


URBN Dental is at your service to provide professional dental tips and quality service. Do you ever wonder how often you should be changing your toothbrush (or toothbrush head if you are using an electric one)? Switching your electric head or tossing your toothbrush is recommended every three months. If you are sick or have a cold sore or canker sore, it’s highly suggested to also switch your brushes. The toothbrush bristles can contain a lot of harmful bacteria and need to be replaced to decrease your risk of potential systemic illnesses. Also the bristles themselves can get worn and frayed and will decrease the efficiency of the toothbrush. Without replacing the toothbrush bristles, you suffer from a greater risk of encountering gum disease and cavities, so be sure you swap those bristles! Schedule a dental appointment now to learn more! Click on our website to book today: https://www.urbndental.com/

Follow one family's journey through the agony of waiting for a donor, a 31-hour surgery, and the prospect of a long road to recovery.
➡ Watch the full documentary here: https://youtu.be/fFua9-Rc4pw
➡ Access our digital archive by becoming a member of National Geographic: https://on.natgeo.com/39wAStK
#NationalGeographic #KatieStubblefield #FaceTransplant
About National Geographic:
National Geographic is the world's premium destination for science, exploration, and adventure. Through their world-class scientists, photographers, journalists, and filmmakers, Nat Geo gets you closer to the stories that matter and past the edge of what's possible.
Get More National Geographic:
Official Site: http://bit.ly/NatGeoOfficialSite
Facebook: http://bit.ly/FBNatGeo
Twitter: http://bit.ly/NatGeoTwitter
Instagram: http://bit.ly/NatGeoInsta
TikTok: http://www.tiktok.com/@natgeo
Tenor: http://on.natgeo.com/31b3Koc
To learn more, please read on here:
https://on.natgeo.com/2vQE1SO
Youngest Face Transplant Recipient in U.S. | National Geographic https://youtu.be/quU9s7I1NLI
National Geographic
https://www.youtube.com/natgeo

Laser-assisted in situ keratomileusis (LASIK) eye surgery can correct or improve your sight by using a laser to change the shape of the cornea. Find out more here: https://www.bupa.co.uk/health-....information/eyes-sig and https://www.bupa.co.uk/health-....information/eyes-sig/laser-eye-surgery
The content is intended for general information only and does not replace the need for personal advice from a qualified health professional.
