- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Learn how LifeVac works through this training demonstration.
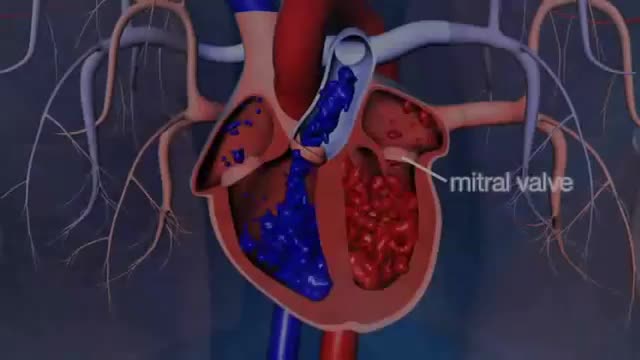
Dr. Glenn Barnhart explains the symptoms of mitral valve regurgitation such as becoming short of breath. There are five structures of the mitral valve: annulus, leaflet tissue, chordae tendineae, papillary muscles, and left ventricle. All of these are taken into consideration when the mitral valve is leaking and not working right. There are four degrees of mitral valve regurgitation: mild, moderate, moderately severe,.
Impaired awareness of illness (anosognosia) is a major problem because it is the single largest reason why individuals with schizophrenia and bipolar disorder do not take their medications. It is caused by damage to specific parts of the brain, especially the right hemisphere.

HPV causes genital warts and cervical and other anogenital cancers. The HPV vaccine is recommended for girls and women 9 to 26 years of age to reduce infections, but information on safety in pregnant women is limited.

In the Womb - Identical Twins
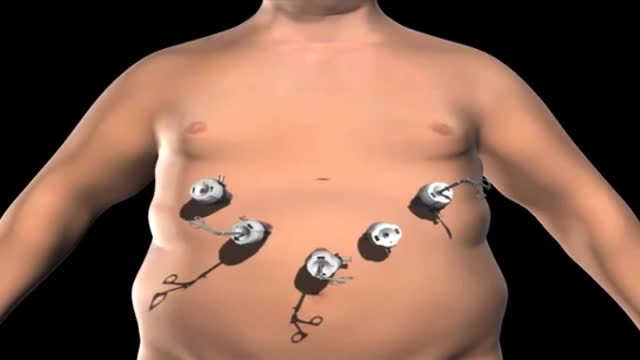
Super Obese individuals (people with a Body Mass Index over 45) have an increased risk during any surgery. And the longer the time under anesthesia, the greater the risk. Gastric bypass surgery can last over 2 hours. Duodenal switch surgery often takes over 4 hours. That’s a long time to be under anesthesia.
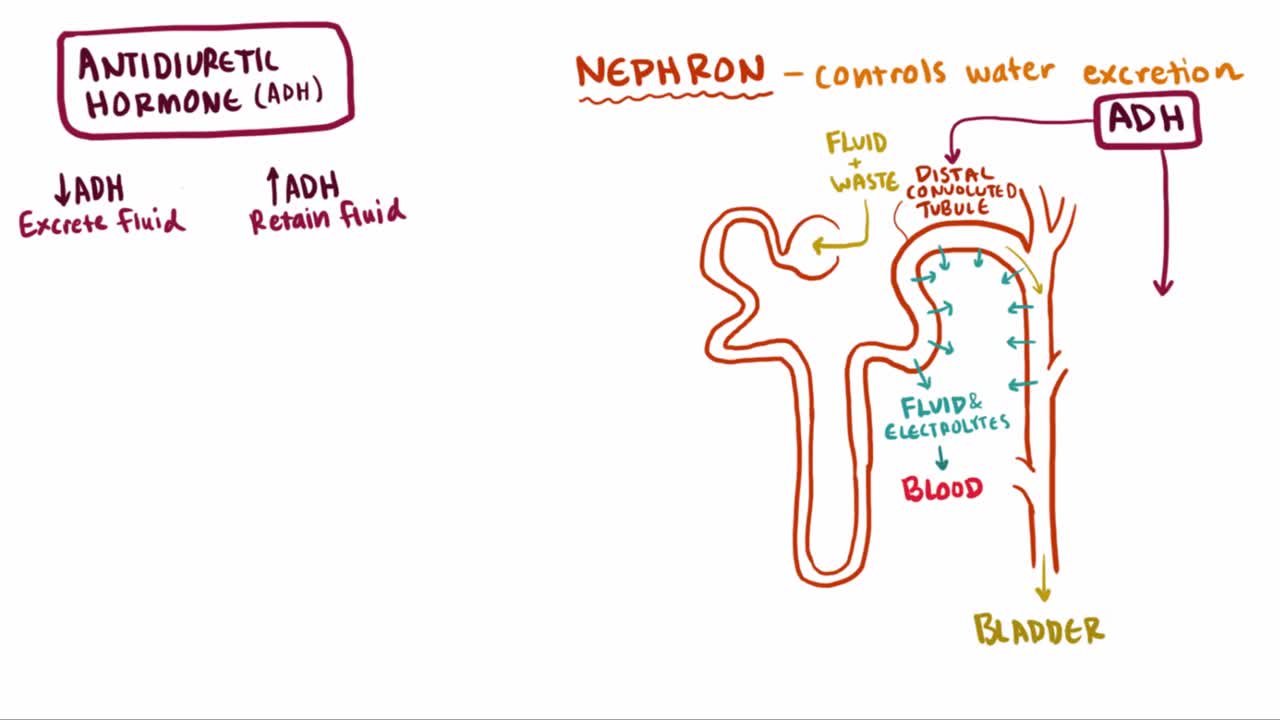
What is syndrome of inappropriate antidiuretic hormone (SIADH)? Well, SIADH is a condition where too much ADH hormone is released, which causes an increase in blood volume and ultimately leads to a series of complications related to the blood osmolality and osmolarity
Gitelman syndrome is a kidney disorder that causes an imbalance of charged atoms (ions) in the body, including ions of potassium, magnesium, and calcium. The signs and symptoms of Gitelman syndrome usually appear in late childhood or adolescence. Common features of this condition include painful muscle spasms (tetany), muscle weakness or cramping, dizziness, and salt craving. Also common is a tingling or prickly sensation in the skin (paresthesias), most often affecting the face. Some individuals with Gitelman syndrome experience excessive tiredness (fatigue), low blood pressure, and a painful joint condition called chondrocalcinosis. Studies suggest that Gitelman syndrome may also increase the risk of a potentially dangerous abnormal heart rhythm called ventricular arrhythmia. The signs and symptoms of Gitelman syndrome vary widely, even among affected members of the same family. Most people with this condition have relatively mild symptoms, although affected individuals with severe muscle cramping, paralysis, and slow growth have been reported.
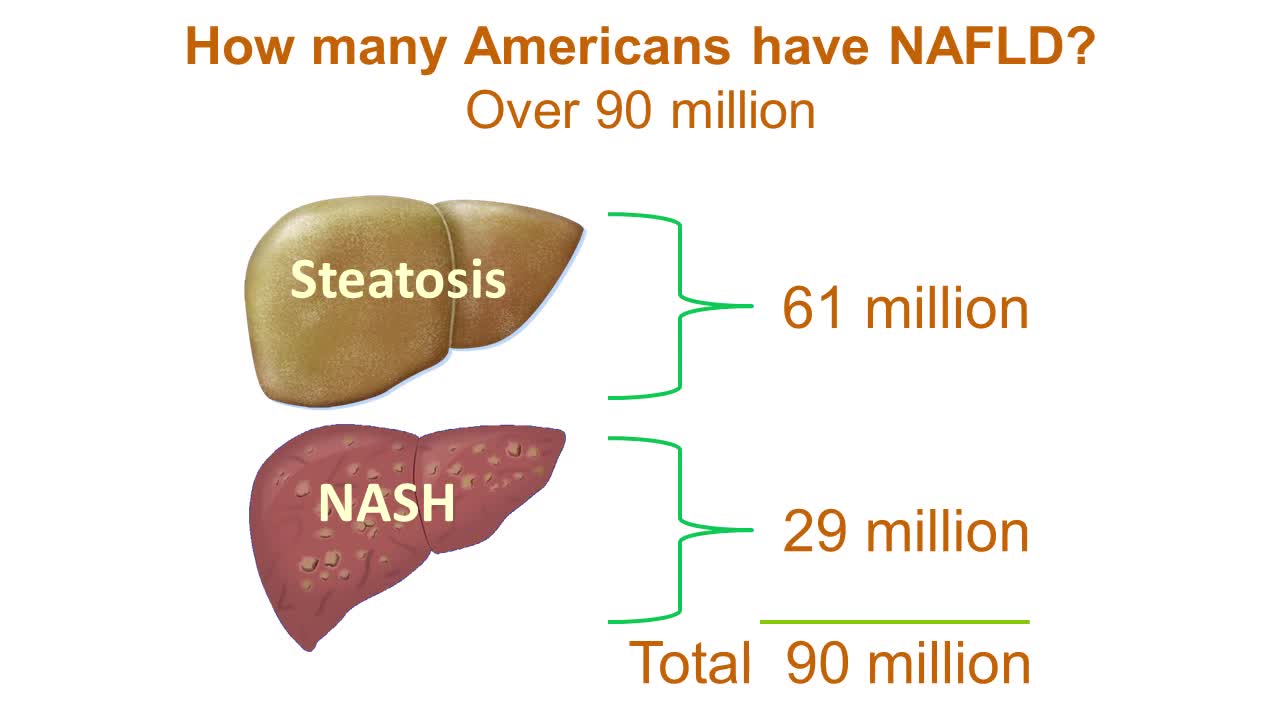
Nonalcoholic fatty liver disease is an umbrella term for a range of liver conditions affecting people who drink little to no alcohol. As the name implies, the main characteristic of nonalcoholic fatty liver disease is too much fat stored in liver cells. Nonalcoholic steatohepatitis, a potentially serious form of the disease, is marked by liver inflammation, which may progress to scarring and irreversible damage. This damage is similar to the damage caused by heavy alcohol use. At its most severe, nonalcoholic steatohepatitis can progress to cirrhosis and liver failure Nonalcoholic fatty liver disease is increasingly common around the world, especially in Western nations. In the United States, it is the most common form of chronic liver disease, affecting an estimated 80 to 100 million people. Nonalcoholic fatty liver disease occurs in every age group but especially in people in their 40s and 50s who are at high risk of heart disease because of such risk factors as obesity and type 2 diabetes. The condition is also closely linked to metabolic syndrome, which is a cluster of abnormalities including increased abdominal fat, poor ability to use the hormone insulin, high blood pressure and high blood levels of triglycerides, a type of fat. Nonalcoholic fatty liver disease care at Mayo Clinic Request an Appointment at Mayo Clinic Symptoms & causes Aug. 23, 2016 Print Share on: Facebook Twitter References Related Magnetic resonance elastography Nonalcoholic fatty liver disease Overview Symptoms & causes Diagnosis & treatment Diagnosis Treatment Departments & specialties Expertise & rankings Locations, travel & lodging Clinical trials Research Costs & insurance Preparing for your appointment Self-management More about In-Depth Multimedia Resources News from Mayo Clinic Advertisement
Hemothorax is the presence of blood in the pleural space. The source of blood may be the chest wall, lung parenchyma, heart, or great vessels. Although some authors state that a hematocrit value of at least 50% is necessary to differentiate a hemothorax from a bloody pleural effusion, most do not agree on any specific distinction. Hemothorax is usually a consequence of blunt or penetrating trauma. Much less commonly, it may be a complication of disease, may be iatrogenically induced, [1] or may develop spontaneously. [2] Prompt identification and treatment of traumatic hemothorax is an essential part of the care of the injured patient. The upright chest radiograph is the ideal primary diagnostic study in the evaluation of hemothorax (see Workup). In cases of hemothorax unrelated to trauma, a careful investigation for the underlying source must be performed while treatment is provided.
This is a demonstration of the scapula manipulation method of relocating a dislocated shoulder

This video demonstrates a technique for reducing a dislocated hip. This patient had recurrent dislocations of his artificial hip.

With so many antibiotics available, it isn't possible to list all of them here. But common antibiotics that are generally considered safe during pregnancy include penicillins (such as amoxicillin and ampicillin), cephalosporins (such as cephalexin), and erythromycin.

The hepatitis A virus, which causes the infection, usually is spread when a person ingests even tiny amounts of contaminated fecal matter. The hepatitis A virus infects liver cells and causes inflammation. The inflammation can impair liver function and cause other signs and symptoms of hepatitis A. Hepatitis A virus can be transmitted several ways, such as: Eating food handled by someone with the virus who doesn't thoroughly wash his or her hands after using the toilet Drinking contaminated water Eating raw shellfish from water polluted with sewage Being in close contact with a person who's infected — even if that person has no signs or symptoms Having sex with someone who has the virus

There is any chance that the snake is venomous The person has difficulty breathing There is loss of consciousness If you know the snake is not venomous, treat as a puncture wound. 1. Note the Snake's Appearance Be ready to describe the snake to emergency staff. 2. Protect the Person While waiting for medical help: Move the person beyond striking distance of the snake. Have the person lie down with wound below the heart. Keep the person calm and at rest, remaining as still as possible to keep venom from spreading. Cover the wound with loose, sterile bandage. Remove any jewelry from the area that was bitten. Remove shoes if the leg or foot was bitten. Do not: Cut a bite wound Attempt to suck out venom Apply tourniquet, ice, or water Give the person alcohol or caffeinated drinks or any other medications
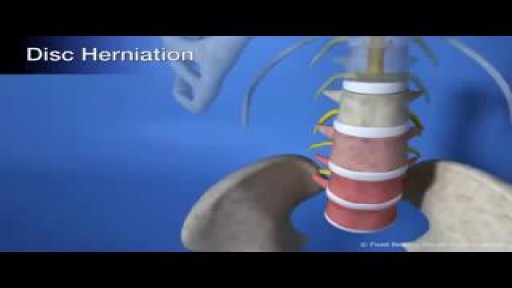
Decompression is a surgical procedure that is performed to alleviate pain caused by pinched nerves (neural impingement). During a lumbar decompression back surgery, a small portion of the bone over the nerve root and/or disc material from under the nerve root is removed to give the nerve root more space and provide a better healing environment. There are two common types of spine surgery decompression procedures: Microdiscectomy Lumbar Microdiscectomy Microdiscectomy Surgery Video A microdiscectomy (a microdecompression) is typically performed for pain from a lumbar herniated disc. The surgery is considered reliable for leg pain caused by the herniated disc, most commonly called sciatica by patients, and most commonly referred to by medical practitioners as a radiculopathy. Read more about Microdiscectomy Surgery

Watch as this wireless brain implant allows a paralyzed monkey to walk again

Male babies leave their DNA in the mother
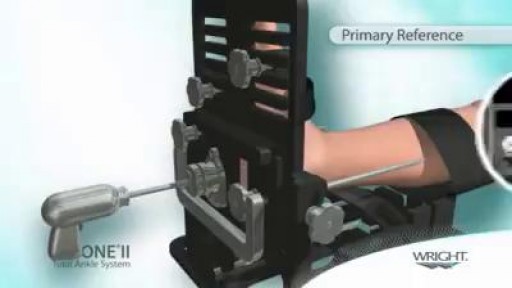
TAA is performed either under general anesthetic or nerve block. A tourniquet is used at the time of surgery to control bleeding and improve visualization during the surgery. The ankle is approached from the front or the side depending on the type of implant being used. Bone is then cut, allowing for placement of the metal and plastic components that re-create the ankle joint. Sometimes the patient will have a tight calf muscle or tight Achilles tendon that needs to be lengthened to improve range of motion of the ankle. The wounds are then closed using stitches or staples, and a splint is applied. A period of non-weightbearing in either a cast or cast boot is necessary to allow the implants to heal in place.

Shigellosis is a diarrheal disease caused by a group of bacteria called Shigella. Shigella causes about 500,000 cases of diarrhea in the United States annually 1. There are four different species of Shigella:
