- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

(cryptorchidism) is a testicle that hasn't moved into its proper position in the bag of skin hanging below the penis (scrotum) before birth. Usually just one testicle is affected, but about 10 percent of the time both testicles are undescended. An undescended testicle is uncommon in general, but common among baby boys born prematurely. The vast majority of the time, the undescended testicle moves into the proper position on its own, within the first few months of life. If your son has an undescended testicle that doesn't correct itself, surgery can relocate the testicle into the scrotum.

After their parents were strongly urged by their local hospital to go to Children's Hospital of Michigan, Dr. Jeffrey Taub controls an aggressive cancer in 2 month old twins. ~ Detroit Medical Center
Watch that video to know about the Health Benefits from KISSING

WORLD'S FIRST IMMEDIATE ROOT-ANALOG ZIRCONIA DENTAL IMPLANT amazing video

Watch that video of an Ingrown hair turns into 140-pound tumor in man’s stomach

Dr. Kathryn Baerman is a Board Certified General Surgeon specializing in Women's Health and Breast Care. She shares with us that in women, hernias present differently than in men. If you are experiencing groin pain, it may be a hernia.
To visit Dr. Baerman in Apex, Chapel Hill, or Durham, North Carolina, call 919-281-1699 to schedule an appointment with her at EmergeOrtho.

Professional breast exam
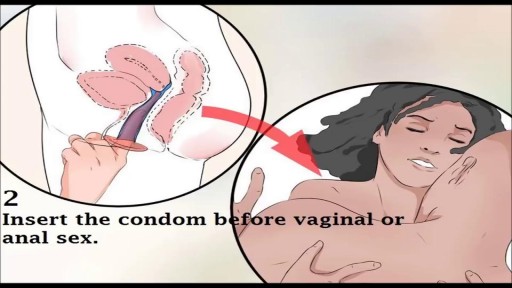
Watch that video to know How to Use Female Condom
This 21 years old man lost his right thumb during a street fight sword blow. the video was taken 3 months after replantation. You can see another videos in my site: https://drliaghatclinic.com, https://instagram.com/liaghatclinic, https://t.me/liaghatclinic

LASIK eye surgery has been popular for more than 20 years, with an estimated 20 million Americans undergoing the procedure to correct nearsightedness and improve distance vision. But some patients says the surgery has ruined their eyesight. Now an expert who once backed LASIK is campaigning to get it off the market. Dr. Tara Narula reports.
Watch "CBS This Morning" HERE: http://bit.ly/1T88yAR
Download the CBS News app on iOS HERE: https://apple.co/1tRNnUy
Download the CBS News app on Android HERE: https://bit.ly/1IcphuX
Like "CBS This Morning" on Facebook HERE: http://on.fb.me/1LhtdvI
Follow "CBS This Morning" on Twitter HERE: http://bit.ly/1Xj5W3p
Follow "CBS This Morning" on Instagram HERE: http://bit.ly/1Q7NGnY
Get new episodes of shows you love across devices the next day, stream local news live, and watch full seasons of CBS fan favorites anytime, anywhere with CBS All Access. Try it free! http://bit.ly/1OQA29B
Each weekday morning, "CBS This Morning" co-hosts Gayle King, Anthony Mason and Tony Dokoupil deliver two hours of original reporting, breaking news and top-level newsmaker interviews in an engaging and informative format that challenges the norm in network morning news programs. The broadcast has earned a prestigious Peabody Award, a Polk Award, four News & Documentary Emmys, three Daytime Emmys and the 2017 Edward R. Murrow Award for Best Newscast. The broadcast was also honored with an Alfred I. duPont-Columbia Award as part of CBS News division-wide coverage of the shootings at Sandy Hook Elementary School in Newtown, Connecticut. Check local listings for "CBS This Morning" broadcast times.

Watch that video of Disgusting! Parasites, zits, insects in people’s ears & more

Funny Video from hospital waiting room

Dr. Joseph McGinn explains minimally invasive bypass, the procedure he pioneered as an alternative to open heart surgery.
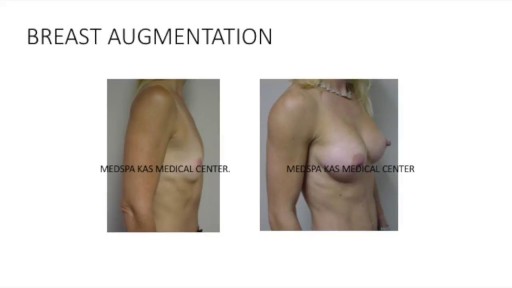
This is a complete video of breast augmentation procedure with implants also includes some before after photographs of breast augmentation surgery by Dr. Ajaya Kashyap at MedSpa Clinic, Delhi, India. source: https://www.youtube.com/watch?v=tRg3RkvCvOE Get more information: www.bestbreastsurgeryindia.com Get more information: www.themedspa.us Email at: info@themedspa.us Call/WhatsApp on:+91-9818369662, 9958221983/82/81

Signs Of Heart Attack In Women, Healthy Habits, What To Do When Someone Is Having A Stroke.--- http://grow-younger-blood.good-info.co --- High Blood Pressure Cured In 9 Minutes Is it possible to drop your high blood pressure below 120/80 in just 9 minutes? Unbelievable…but the answer is YES! Not only is it possible…thousands of people have done it already. In fact, this little technique has become the #1 “underground” high blood pressure trend of the year. And we’re expecting it to become mainstream very soon. What’s more…this method requires NO pills, supplements, diets, or strenuous workouts. I explain this all here in today’s video… http://grow-younger-blood.good-info.co

The most reliable clinical sign to detect ascites is checking for bilateral flank dullness. If a patient with ascites is lying supine, fluid accumulates in the flank regions, leading to dullness on percussion. At the same time, the air-filled bowel loops are forced upwards by the free fluid due to buoyancy, resulting in tympanitic percussion. To locate specifically where dullness shifts to tympany, or the air-fluid level, percussion should be performed from the sides towards the middle. To confirm that the dullness is caused by ascites, ask the patient to switch to a lateral decubitus position. If ascites is present, the air-filled bowel loops will shift accordingly and remain at the surface of the fluid. As a result, the air-fluid level will shift as well. This is known as shifting dullness.
Subscribe to AMBOSS YouTube for the latest clinical examination videos, medical student interviews, study tips and tricks, and live webinars!
Free 5 Day Trial: https://go.amboss.com/amboss-YT
Instagram: https://www.instagram.com/amboss_med/
Facebook: https://www.facebook.com/AMBOSS.Med/
Twitter: https://twitter.com/ambossmed
Blog: https://blog.amboss.com/us
#AMBOSSMed #ClinicalExamination

An ectopic pregnancy (EP) is a condition in which a fertilized egg settles and grows in any location other than the inner lining of the uterus. The vast majority of ectopic pregnancies are so-called tubal pregnancies and occur in the Fallopian tube.

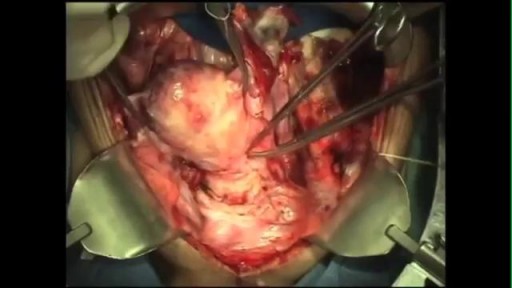
laparoscopic left adrenalectomy in 150kg patient with Cushings

Loyola Full Male Exam Part 4 A video from Loyola medical school, Chicago showing the full examination of the male
